Anatomy of the muscles of the human neck and head: structure and functions. The superficial muscles of the neck are derivatives of the branchial arches. The muscles of the neck include the muscle
The muscles of the neck refer to a large array of superficial and deep muscles.
They perform several functions: keeping the head in balance, helping with swallowing and pronouncing sounds, and ensuring movement of the neck and head.
Pain in the neck muscles can be a symptom of diseases such as myositis, fibromyalgia, myofascial syndrome.
Those who care about their health will find it useful to familiarize themselves with the anatomy of the neck muscles.
In medical practice, the neck muscles are divided into superficial and deep.
Both groups include several muscles, each of which is responsible for performing specific functions.
Superficial muscles
This muscle group consists of 2 parts: the subcutaneous muscle and the sternocleidomastoid muscle..
Sternocleidomastoid

Represents long splenius muscle with two heads. At birth, this muscle can be damaged and partially replaced by fibrous tissue. The latter shrinks and forms torticollis (a disease associated with curvature of the neck).
Muscle arises from the sternal head(anterior surface of the manubrium of the sternum) and clavicular head(upper surface of the middle third of the clavicle). The place of its attachment is the mastoid process of the temple bone, or rather the outer surface of this process.
If both halves contract, the muscle pulls the head forward and bends the neck(for example, this happens when you try to lift your head from the pillow). When you inhale deeply, it lifts the ribs and sternum up. If one half contracts, the muscle tilts the head forward on the side of contraction. Responsible for rotating the head up and in the opposite direction.
Subcutaneous
Specified muscle located just under the skin, is flat and thin. It begins in the chest area below the collarbone, passes medially and upward, occupying almost the entire anterolateral area of the neck. Only a small triangle-shaped area located above the jugular notch remains unclosed.
Bundles of the subcutaneous muscle rise into the facial area and are woven into the masticatory fascia. Some of them attach to the laughter muscle and the muscle that depresses the lower lip.
This muscle pulls back the skin and protects the veins from compression. It can also pull the corners of the mouth down, which is important for human facial expressions.

Middle muscles
The middle or median muscles of the neck are suprahyoid and infrahyoid.
Mylohyoid muscle
Has the shape of an irregular triangle, is flat. It begins in the area of the lower jaw, where the mylohyoid line is located. The muscle bundles go from top to bottom, as well as from back to front.
When they reach the midline, they connect with bundles of the same muscle on the opposite side and form a suture of the mylohyoid muscle. The posterior bundles join the anterior portion of the hyoid bone. The left and right mylohyoid muscles form the floor of the mouth and are called the diaphragm of the mouth.
The main task of the mylohyoid muscle is to lift the hyoid bone upward. If the muscle is fixed, it helps lower the movable (lower) jaw and is an antagonist of the masticatory muscles. When the muscle contracts while eating, it lifts and presses the tongue against the roof of the mouth, allowing the bolus of food to pass into the throat.
Digastric
The digastric muscle is the tendon that connects the posterior and anterior belly and is attached to the greater horn and body of the hyoid bone using a fascial loop.
The digastric muscle helps with active opening of the mouth (with resistance, for example), lowering the lower jaw while the hyoid bone is fixed.
When swallowing she elevates the hyoid bone to the mastoid process and mandible(if the latter is fixed by the masticatory muscles). The muscle is capable of moving the hyoid bone back when the posterior abdomen contracts. Since the hyoid bone does not form joints with other bones, we can say that it is displaced relative to the soft tissues.
Video: "Neck triangles"
Stylohyoid muscle
Has a thin, flattened abdomen, starting in the area of the styloid process of the temporal bone, going forward and down, located along the digastric muscle (the anterior surface of its posterior abdomen). The distal end of the muscle splits, covers the tendon of the digastric muscle with legs, and is attached to the greater horn, the body of the hyoid bone.
Like the rest of the muscles located above the hyoid bone, the stylohyoid muscle is a component of a complex apparatus. This apparatus includes the hyoid bone, lower jaw, trachea, larynx and plays an important role in the process of articulate speech.
Sternohyoid
Located deep. The function of the muscle is to lower the hyoid bone. When the suprahyoid muscles (located between the mobile jaw and the hyoid bone) contract, the sternohyoid muscle, together with the maxillary and sternothyroid muscles, moves the lower jaw.
This function is not included in the table of antagonists and synergists, since this function does not have a direct effect on the temporomandibular joint.
Geniohyoid
It begins in the area of the mental axis of the lower jaw, then goes down and back. Located above the mylohyoid muscle, it is attached to the body of the hyoid bone (its anterior surface).
Raises the hyoid bone upward. To a fixed state, it helps to lower the movable jaw, which makes it an antagonist of the masticatory muscles.
Scapular-hyoid
Did you know that...
Next fact
It is part of the sublingual muscle group and is a paired muscle on the anterior surface of the neck. It has a long, flattened shape and a tendon that divides it into two abdomens.
The scapulohyoid muscle pulls down the hyoid bone and provides tension on the pretracheal plate of the cervical fascia.
Sternothyroid
The sternothyroid muscle has a flat shape. It originates from the posterior surface of the first cartilage and the manubrium of the sternum, goes upward and attaches to the thyroid cartilage of the larynx (an oblique line of its lateral surface). The main task of this muscle is to lower the larynx.
Thyrohyoid
It starts from the oblique line of the thyroid cartilage. Attached to the greater horn, the body of the hyoid bone. Raises the larynx with the hyoid bone fixed.

Muscles deep
The deep neck muscles are a complex of lateral and medial (prevertebral) muscles. The list of deep tissues includes the anterior, posterior, middle scalene muscles, longus colli muscle; lateral rectus, anterior rectus and longus capitis muscles.
Anterior scalene muscle
Originates from the anterior tubercles of the third and fourth cervical vertebrae, goes down and forward, attaches to the anterior scalene muscle of the first rib in front of the groove of the subclavian artery.
This muscle plays an important role in the functioning of the body. She provides elevation of the upper rib during breathing, turning the neck in different directions, bending the cervical part of the spinal column forward.
Middle staircase
It begins in the area of the posterior tubercles of the six lower vertebrae of the neck, goes down behind the anterior scalene muscle and is attached to the upper surface of the 1st rib, behind the groove of the subclavian artery.
Above this groove, between the middle and anterior scalene muscles, there is a triangular gap in which the nerve trunks of the brachial plexus, as well as the subclavian artery, pass.
The middle scalene muscle acts as an inspiratory muscle(raises the first upper rib). With fixed ribs, it contracts on both sides and bends the cervical part of the spinal column forward. With a unilateral contraction, it bends the same part of the spine and turns it to the left or right.
Rear staircase
It originates from the transverse processes of the 6th, 5th, 4th and 3rd cervical vertebrae, moves down behind the middle scalene muscle, and is attached to the outer surface of the second rib.
The posterior scalene muscle acts as an inspiratory muscle. With fixed ribs, it bends the cervical spine anteriorly (since it contracts on both sides). With unilateral contraction, it bends and turns this section in a certain direction.
Longus colli muscle
Occupies the entire anterolateral surface of the vertebral bodies, from the atlas to the 3rd and 4th thoracic vertebrae. The middle sections of the muscle are slightly expanded. The length of the muscle bundles varies, so the muscle is usually divided into three parts: superior oblique, medial vertical, inferior oblique.
Longus capitis muscle
Located in front of the longus colli muscle. The origin is the transverse processes from the 3rd to 6th cervical vertebrae. The place of attachment is the occipital bone (the muscle is located in front of the foramen magnum of this bone).
The function of the longus muscle is to tilt the head and flex the upper half of the cervical spine.
Rectus capitis anterior muscle
This neck muscle is short. It begins where the lateral mass of the atlas and the anterior surface of the transverse process are located. From here the muscle goes up and is attached to the bottom of the basilar part of the occipital bone, in front of the foramen magnum.
The task of the muscle is to tilt the head in one direction or another(unilateral contraction) or tilt your head forward (bilateral contraction).
Lateral rectus capitis muscle
The origin of the muscle is the anterior part of the transverse process of the atlas.. From here the beams are directed outward and upward. The muscle ends in the area of the paramastoid process of the jugular process of the occipital bone.
The function of the lateral rectus muscle depends on the type of contraction. With unilateral contraction, it tilts the head to the side, and with bilateral contraction, it tilts forward..

What diseases of the neck muscles are there?
The most common diseases of the neck muscles include:
- Myofascial syndrome. The disease is widespread in clinical practice. May be accompanied by neck pain, numbness in the hands and other unpleasant symptoms. Usually seen in people who have to stay in the same position for a long time. Prolonged tension leads to muscle spasms. Spasmed areas transform into lumps and lumps (trigger points).
- Myositis. Occurs due to being in a draft for a long time. The peak incidence occurs in the summer and spring, when most homes and offices have open windows or air conditioners. Cold air irritates the nerve endings located in the skin. The latter send a nerve impulse to the brain, thereby triggering a chain reaction, causing painful muscle contracture.
- Fibromyalgia. It is a chronic disease. It is characterized by increased sensitivity and soreness of muscles, tendons, and joints.
Video: "Anatomy of the neck muscles"
Conclusion
Thus, neck muscles- This is a complex mechanism consisting of several muscle groups. These include deep, superficial, and median muscles. Each group is responsible for performing certain functions. When muscles are exposed to negative environmental influences (cold) or remain in the same position for a long time, various diseases occur. Knowing the anatomy of the neck muscles and following preventive recommendations will help avoid the development of diseases and their complications.
In case of fractures of the lower jaw, the function of each of the masticatory muscles is realized differently than normally, and depends on how the fracture line passes. So, if the fracture line passes through the neck of the lower jaw, then the superficial part of the masticatory muscle and the medial pterygoid muscle displace the lower jaw (without condylar processes) anteriorly and upward.
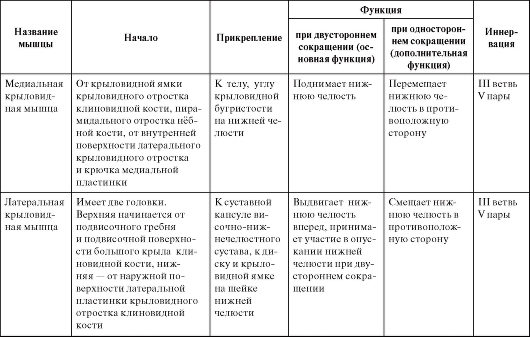
Table 10. Muscles involved in movements of the lower jaw
Continuation of the table. 10
End of table. 10

Typical features of the masticatory muscles
The superficial layer of the masticatory muscle in brachycephaly and chameprosopic facial shape is usually wide and low, the muscle fibers diverge downward (Fig. 85); with dolichocephaly and leptoprosopic face shape, it is long and narrow, the muscle fibers run parallel. The intermediate layer of this muscle in dolichocephaly and leptoprosopia protrudes more from under the posterior edge of the superficial layer than in brachycephaly and chameprosopia.
The temporal muscle with a dolichocephalic form of the skull is low and long, and with a brachycephalic form it is high and short (see Fig. 85).
Both heads of the lateral pterygoid muscle with a brachycephalic form of the skull are short and wide, with a narrow gap between them, with a dolichocephalic form they are long and narrow, with a wide gap between them (Fig. 86).
The medial pterygoid muscle with a dolichocephalic shape of the skull and a leptoprosopic shape of the face is long and narrow, and with brachycephaly and chameprosopia it is low and wide (Fig. 87).
The shape of the pterygoid and masseter muscles is determined by the shape of the ramus of the mandible and the infratemporal fossa, but at the same time it corresponds to the structure of the bone components of the temporomandibular joint. This connection is especially clearly reflected in the external structure of the lateral pterygoid muscle. When opening the mouth (lowering the lower jaw) and when moving the lower jaw forward in people with a brachycephalic skull, the head of the joint moves to the top of the flat articular tubercle, i.e. the articular path deviates little from the horizontal plane. This movement of the head of the jaw is ensured by the lower head of the lateral pterygoid muscle, which lies almost horizontally. With a dolichocephalic form of the skull, the articular head slides downward rather than horizontally along the steep and high slope of the articular tubercle. This movement is provided by the lower head of the lateral pterygoid muscle, the beginning of which is located lower on the high lateral plate of the pterygoid process, and the muscle pulls the head of the jaw downward rather than forward.
1. M. platysma, subcutaneous muscle of the neck, lies directly under the skin on the fascia in the form of a thin plate. It begins at the level of the second rib from the fascia pectoralis et deltoidea and is attached to the edge of the lower jaw and to the fascia parotdea et fascia masseterica, partly continuing into the muscles of the mouth. (Inn. n. facialis.)
Function. By pulling the skin of the neck, the muscle protects the saphenous veins from compression; in addition, she can pull the corner of her mouth down, which is important in facial expressions.
2. M. sternocleidomastoides, sternocleidomastoid muscle, lies immediately under the previous one, separated from it by the cervical fascia. It starts from the manubrium of the sternum and from the sternal end of the clavicle and attaches to the mastoid process and to the linea nuchae superior of the occipital bone. By its origin, the muscle represents a separated part of m. trapezius and therefore has the same innervation with this muscle (n. accessorius and CII).
Function. With unilateral contraction, the muscle tilts the cervical spine in its direction; At the same time, the head is raised with the face rotated in the opposite direction.
With bilateral contraction, the muscles hold the head in an upright position, therefore the muscle itself and the place of its attachment (processus mastoideus) are most developed in humans in connection with upright posture. With bilateral contraction, flexion of the cervical spine with simultaneous elevation of the face can also occur. When the head is fixed, it is possible to raise the chest during breathing (auxiliary inspiratory muscle).


According to the topographic classification, all cervical muscles are divided into the following groups: superficial, deep. A distinctive feature of the latter is its location next to the spinal column: they are responsible for turns and tilts of the cervical vertebrae. But the muscles of the superficial neck are involved in the process of chewing, swallowing, and allow you to pronounce sounds. This group includes different muscles, each of them has its own characteristics of location, blood supply, innervation and its own functionality.
Types of superficial muscles
The superficial cervical muscles include the suprahyoid and infrahyoid groups. They include muscles that attach to or near the hyoid bone and allow it to move (forward, down, up). The following muscles also belong to the superficial:
- Subcutaneous
It is located just under the skin of the neck in the front. It has a small thickness and is completely flat. Runs from the collarbone to the hyoid bone (but does not lie under the jugular notch). Due to a slight divergence at the top, it is attached to several other muscles responsible for the movement of the lips. Therefore, its main functions include lowering the corners of the mouth, as well as protecting the veins of the neck from compression (responsible for “holding” the skin above them).
- Sternocleidomastoid
Located directly under the subcutaneous muscle. It rises from the sternal ends of the clavicles/manubrium of the sternum (each branched into two parts at the ends). It is a steam room: it is located on both the left and right sides of the neck. At the top it is attached to the temporal mastoid process. Its most important functions include turning the head, tilting it, and throwing it back. The auxiliary function as a respiratory muscle appears when the head is in a fixed position.
The remaining groups (suprahyoid and subhyoid) have a more precise demarcation and directly connect to the hyoid bone. They differ from the considered types of muscles not only in topography, but also in the characteristics of blood supply and innervation.
Functions of superficial muscles
The suprahyoid muscle group, due to its specific location and attachment, is responsible for connecting the hyoid bone with the trachea, pharynx, base of the skull and lower jaw. Therefore, its main functions of different muscles of the group include:
- movement of the hyoid bone and lowering of the lower jaw (digastric);
- movement of the hyoid bone upward or backward (stylohyoid);
- simultaneous raising of the hyoid bone along with the larynx in conditions of clenching the jaws or lowering the lower jaw for speaking, chewing or swallowing (mylohyoid, geniohyoid).
Despite the similar functionality of different types of muscles, their work is ensured in a complex manner. In addition, the suprahyoid group is distinguished by its close connection with the adjacent muscles of the pharynx and tongue. The main functions performed by another group - the sublingual - include:
Shifting the hyoid bone downwards, to the side, according to the tension of the paired omohyoid muscle attached to it. Thanks to the tension of the middle cervical fraction, compression of the deep cervical veins is prevented. The last special function is caused by the need to regulate tension due to increased blood flow to the veins in the chest cavity from the veins of the neck during inhalation.
The downward movement of the hyoid bone is ensured by the joint work of the sternohyoid, digastric, and mylohyoid muscles.
The hyoid bone is brought closer to the larynx by means of the thyrohyoid muscle. But the nearby sternothyroid one pulls the larynx itself down. It is also responsible for the movement of the thyroid cartilage and larynx.
With the joint contraction of different sublingual muscles, the hyoid bone is strengthened and the lower jaw is subsequently lowered. The specificity of the connection of the subhyoid muscles with the hyoid bone is also important. They are attached to it from below, departing immediately from the sternum or shoulder blades, cartilage of the larynx. This location feature ensures the functions performed by this group.
The retention and movement of the hyoid bone is ensured exclusively by the complex work of different muscle groups. They are a kind of counterweight relative to each other, allowing chewing, making sounds and even simply moving the lower jaw.
Features of blood supply
The specificity of the blood supply to different types of superficial neck muscles is determined according to their location and attachment. For example, the superior saphenous muscle receives its blood supply from the superficial and facial arteries. But for the sternocleidomastoid, located slightly deeper, the blood supply is carried out from the branches of the occipital, superior thyroid artery.

For the suprahyoid group, blood supply is also provided from different arteries. Blood supply to the digastric muscle is carried out for the anterior and posterior abdomen by separate arteries, namely: the mental (for the anterior) and the occipital, the posterior auricular (for the posterior). The blood supply to the stylohyoid muscle is provided from both the facial and occipital arteries due to its specific attachment. And for the maxillary-hyoid, geniohyoid muscle, the blood supply is from the mental artery. But blood supply to the geniohyoid muscle can also be provided from the hypoglossal artery.
As for the subhyoid muscle group, their blood supply comes from the transverse cervical and inferior thyroid artery. This feature of the general blood supply of the group is determined by their close location and fairly close attachment next to each other.
Innervation of superficial muscles
Both the blood supply and the innervation for the subhyoid muscle group are similar. In particular, it is produced by the muscular branches of the nerve plexus. They are divided into short and long. For the omohyoid muscle, innervation is provided from the cervical loop CII-CIII. For all other muscles of the group under consideration, the cervical loop CI-CIII is innervating.
For the suprahyoid group, innervation is provided from the branches of the muscular cervical plexus CI-CII, and from the facial nerve VII, and from the mylohyoid nerve, and from the hypoglossal nerve XII. For the subcutaneous muscle, the innervating one is the facial nerve VII, and for the sternocleidomastoid - the accessory nerve XI.
According to this information, one can be convinced of the similarity of the functional capabilities of the superficial muscles, their similar blood supply and innervation (especially for general groups). Therefore, the specifics of the functioning of different muscles from the same group are usually not separated: they all work in a complex manner.
The superficial muscles of the neck include: the subcutaneous neck muscle, the sternocleidomastoid muscle and the muscles attached to the hyoid bone, as well as the suprahyoid and infrahyoid muscles. The group of suprahyoid muscles includes the mylohyoid, digastric, stylohyoid and geniohyoid muscles. The sublingual muscles include the sternohyoid, sternothyroid, thyrohyoid and omohyoid muscles. The deep muscles of the neck are in turn divided into the lateral and prevertebral groups. The lateral group includes the anterior, middle and posterior scalene muscles lying on the side of the spinal column. The prevertebral group, located in front of the spinal column, includes the muscles of the head: the anterior rectus capitis muscle, the lateral rectus capitis muscle, and the longus colli muscle.
The subcutaneous muscle of the neck (platysma) is thin, flat, and lies directly under the skin. It begins in the thoracic region below the clavicle on the superficial plate of the pectoral fascia, passes upward and medially, occupying almost the entire anterolateral region of the neck. A small area in the form of a triangle above the jugular notch of the sternum remains uncovered by the muscle.
The sternocleidomastoid muscle (m. sternocleidomastoideus) is located under the subcutaneous muscle of the neck; when the head is turned to the side, its contour is indicated in the form of a pronounced ridge on the anterolateral surface of the neck. This muscle begins in two parts (medial and lateral) on the anterior surface of the manubrium of the sternum and the sternal end of the clavicle. Rising upward and posteriorly, the muscle attaches to the mastoid process of the temporal bone and the lateral segment of the superior nuchal line of the occipital bone. Above the clavicle, between the medial and lateral parts of the muscle, the small supraclavicular fossa (fossa supraclavicularis minor) stands out.
Muscles attaching to the hyoid bone

The muscles lying above the hyoid bone are distinguished - the suprahyoid muscles (mm. suprahyoidei), and the muscles lying below the hyoid bone - the subhyoid muscles (mm.infrahyoidei). Both groups of muscles (paired) act on the hyoid bone, which is a support for muscles that take part in important functions: acts of chewing, swallowing, speech, etc. The hyoid bone is held in its position solely by the interaction of muscles that approach it from different sides.



: instructions for use")





- What is Shatavari? Can I take Shatavari during menstruation?
- A blow above the belt, or how to treat breast hematomas. Medicines against hickeys.
- Hormones for cats: pros and cons Increased mammary gland size
- How toothpaste appeared and evolved A brief history of toothpaste for children
- Complications after postinoration
- White spots in the mouth on the palate and tongue: why it occurs and how to treat it, what kind of disease
- Neck massage is an excellent way to relieve tension and pain. Strengthening exercises for the neck muscles after surgery.
- Early pregnancy termination methods
- Norkolut for menstruation - the right solution to restore your cycle
- Why do I have discharge a week before my period?
- If your periods come in chunks, what could this mean?
- What does Theraflu help with? When is it better to drink Theraflu?
- The use of eyebright for eye diseases: effective traditional medicine
- Attractions, indications and contraindications, reviews
- Calcium gluconate (solution for injection): instructions for use
- Red brush for women and men
- What is the UHF procedure, its indications and contraindications UHF therapy what is treated
- UHF electric field is an accessible and effective method of physiotherapy for acute inflammatory diseases. What therapeutic effect does UHF therapy have?
- A child has a dry cough: how to treat Komarovsky cough
- Indications, contraindications, reviews