Exercise therapy in diseases of the nervous system of the central and peripheral. Effective treatment of neuroses. Therapeutic exercise for neuroses Exercises for diseases of the nervous system goal
Any motor act occurs when
transmission of impulses along nerve fibers
cerebral cortex to anterior horns
spinal cord and further to the muscles.
In diseases (injuries of the spinal cord)
nervous system conduction of nerves
impulses is difficult, and there is
dysfunction of the muscles.
Complete loss of muscle function
called paralysis (plegia), and
partial - paresis.
According to the prevalence of paralysis, there are:
monoplegia (lack of movement in one limb -arm or leg)
hemiplegia (damage to the upper and lower limbs)
one side of the body: right-sided or left-sided
hemiplegia),
paraplegia (impaired movement in both lower
limbs is called lower paraplegia, in the upper -
upper paraplegia)
tetraplegia (paralysis of all four limbs).
Peripheral nerve damage causes paresis
in the zone of their innervation, called
of the corresponding nerve (for example, paresis of the facial nerve,
paresis of the radial nerve, etc.). Nerves of the upper limb: 1 - radial nerve; 2 - musculocutaneous nerve; 3 - median nerve; 4 -
ulnar nerve.
I - brush with damage to the radial nerve. II - brush with damage to the median nerve.
III - hand with damage to the ulnar nerve The rehabilitation regime should be
adequate to the severity of the disease, which
assessed by the degree of violation
adaptive activity.
The level of damage to the CNS is taken into account and
peripheral nervous system.
Factors such as the ability to
move independently,
serve yourself.
Exercise therapy in neurology has a number of rules
early use of exercise therapy;the use of means and techniques of LG for
restoration of temporarily impaired functions or
for maximum compensation of lost;
selection of special exercises in combination with
general developmental, general strengthening
exercises and massage;
strict individuality of exercise therapy, depending on
diagnosis, age and gender of the patient;
active and steady expansion of motor
mode from the prone position to the transition to
sitting, standing, etc. Special exercises can be conditionally divided into
the following groups:
exercises that increase joint range of motion
and muscle strength
recovery exercises and
improved coordination of movements;
antispastic and antirigid exercises;
ideomotor exercises (sending a mental impulse
to the muscle group being trained)
a group of exercises aimed at restoring or
development of motor skills (standing, walking,
manipulations with simple but important household
objects: clothes, utensils, etc.);
passive and stretching exercises
connective tissue formations, treatment
position, etc. All of the above groups of exercises
combined in various combinations and
depends on:
nature and volume of motor
defect,
stage of rehabilitation
the age and sex of the patient.
Brain injury (concussion)
All brain injuries areincreased intracranial pressure.
For motor dysfunctions
prevention of contractures prescribe exercise therapy
(passive, then passive-active movements,
positioning, stretching exercises
muscles, etc.)
massage of the back and paralyzed limbs
(first massage the legs, then the arms, starting with
proximal parts)
and also affect biologically active
limb points.
Injuries of the spine and spinal cord
The clinical course of the disease depends on the degreelesions of the spinal cord and its roots.
So, with injuries of the upper cervical region
spinal spastic tetraparesis occurs
limbs.
With lower cervical and upper chest localization
(C6-T4) flaccid hand paresis and spastic
paresis of the legs.
With thoracic localization - paresis of the legs.
With damage to the lower thoracic and lumbar
spinal segments develop flaccid paralysis
legs. Flaccid paralysis can also be caused
be spinal cord injury
closed fractures of the spine and its
wounds.
methodical methods of LG
performance of ideomotor exercises;isometric muscle tension;
water exercises;
choice of starting positions, facilitating
muscles to perform movements;
passive and active-passive
exercises;
use of various devices
reducing weight and friction (blocks and loops,
smooth surfaces, exercise in the water).
Any movement occurs when impulses are transmitted from the cerebral cortex to the anterior horns of the spinal cord. At the same time, it has been proven that normal brain function requires a constant influx of impulses from the periphery: skin, muscles and joints. In diseases and injuries of the central nervous system, the conduction of nerve impulses is difficult, due to a violation of the innervation of the muscles, there are paresis(weakening of voluntary movements) and paralysis(lack of voluntary movements).
When the cells of the anterior horns of the spinal cord and their fibers are damaged, a sluggish(peripheral) paralysis or paresis, accompanied by paresis or paralysis, hypotension or atony of the muscles and hyporeflexia or complete absence of tendon, periosteal and skin reflexes. Sensitivity is often reduced and trophism is disturbed, which can lead to muscle atrophy.
With injuries and diseases of the brain or spinal cord, the inhibitory effect of the cerebral cortex on spinal motor neurons is reduced, and their functions are activated. As a result, there is a central spastic paralysis: increased muscle tone, hyperreflexia, the appearance of pathological reflexes, and on the arm the tone is increased mainly of the flexors and pronators, and on the leg - mainly of the extensors. The patient takes the Wernicke-Mann position: the shoulder is brought to the body, the hand and forearm are bent, the hand is turned palm down, the leg is extended at the knee and hip joints, the foot is bent.
Common for all injuries and diseases of the nervous system are limitation of the range of motion, decreased muscle tone, vegetotrophic disorders, etc.
Physical exercise:
- cause an influx of impulses into the cerebral cortex, which regulates all body functions;
- by activating the motor neurons of the spinal cord, they increase the biopotential of the muscles and restore their functions.
Special exercises conditionally divided into the following groups:
- exercises that increase joint range of motion and muscle strength;
- exercises aimed at restoring and improving coordination of movements;
- antispastic exercises;
- ideomotor exercises (sending a mental impulse to a trained muscle group);
- a group of exercises aimed at restoring or forming motor skills (standing, walking, manipulations with simple household objects - clothes, dishes, etc.);
- passive exercises and exercises for stretching connective tissue formations, treatment with position, etc.
The contusion of the brain in its severity, symptoms and clinical manifestations gives a picture of severe concussion with deep damage. The most common complications of brain contusion include paresis and paralysis of the limbs, hearing, vision, smell, taste, speech and intellect disorders (traumatic dementia).
Breathing exercises and exercises for small and medium muscle groups are prescribed after the cessation of nausea and vomiting, active therapeutic exercises - a few days before the victim is allowed to sit down. With paresis and paralysis, passive therapeutic exercises are prescribed, despite the serious condition of the patient, even in the intensive care unit or intensive care unit.
Contraindications to the use of exercise therapy in neurology:
- exacerbation of ischemic brain disease;
- repeated stroke;
- vascular thrombosis;
- hypertensive crisis;
- pronounced pain syndrome;
- acute encephalitis, myelitis;
- neuritis;
- repeated trauma to the brain and spinal cord;
- exacerbation of concomitant chronic diseases of internal organs;
- acute intercurrent diseases.
Chapter 15 exercise therapy for diseases and injuries of the peripheral nervous system
Neuritis is a disease of peripheral nerves that occurs as a result of traumatic injury, infectious, inflammatory diseases (diphtheria, influenza, etc.), beriberi (lack of B vitamins), intoxication (alcohol, lead) and metabolic disorders (diabetes).
The most common neuritis of the facial nerve, neuritis of the radial, median, ulnar, sciatic, femoral and tibial nerves.
The nature of functional disorders in injuries of the peripheral nerves of the upper and lower extremities is determined by their localization and the degree of damage. The clinical picture in neuritis is manifested by sensitivity disorders (pain, temperature, tactile), motor and vegetotrophic disorders.
Motor disorders in neuritis are manifested in the development of paresis or paralysis.
Peripheral (flaccid) paralysis is accompanied by muscle atrophy, decrease or disappearance of tendon reflexes, muscle tone, trophic changes, skin sensitivity disorders, pain when stretching muscles.
Exercise therapy, massage and physiotherapy occupy an important place in complex rehabilitation treatment.
Tasks of complex rehabilitation treatment for peripheral paralysis:
Stimulation of the processes of regeneration and disinhibition of nerve sections that are in a state of oppression;
Improving blood supply and trophic processes in the lesion in order to prevent the formation of adhesions and cicatricial changes;
Strengthening paretic muscles and ligaments;
Prevention of contractures and stiffness in the joint;
Recovery of working capacity by normalizing motor functions and developing compensatory adaptations.
Exercise therapy is contraindicated in severe pain and severe general condition of the patient. The methodology and nature of rehabilitation measures are determined by the nature of movement disorders, their localization and the stage of the disease.
The following periods are distinguished: early recovery (2-20th day), late recovery, or main (20-60th day), and residual (more than 2 months).
With surgical interventions on the nerves, the time limits of all periods are fuzzy: for example, the early recovery period can last up to 30-40 days, the late one - 3-4 months, and the residual one - 2-3 years.
early recovery period. With the development of paralysis, optimal conditions are created for the restoration of a damaged limb - treatment with position, massage and physiotherapy procedures are used.
Position treatment is prescribed to prevent overstretching of weakened muscles; for this, splints are used that support the limb, special “laying”, corrective positions. Treatment by position is carried out throughout the entire period - with the exception of therapeutic exercises.
feature massage with peripheral paralysis is the differentiation of its effects on the muscles, a strict dosage of intensity, the segmental-reflex nature of the effect (massage of the collar, lumbosacral regions). A beneficial effect is exerted by hardware massage (vibration), carried out at the "motor points" and along the paretic muscles; vortex and jet underwater massage, combining the positive temperature effect of warm water and its mechanical effect on tissues.
In the absence of motor functions, to improve conduction along the nerves, physiotherapy(electrophoresis with calcium ions).
After physiotherapeutic procedures, therapeutic exercises are carried out; with complete paralysis, they mainly consist of passive and ideomotor exercises. It is advisable to combine passive exercises with active movements in the same joints of a symmetrical limb.
During classes, it is especially necessary to monitor the appearance of voluntary movements, choosing the optimal starting positions, and strive to support the development of active movements.
In the late recovery period, positional treatment, massage, therapeutic exercises and physiotherapy are also used.
Position treatment has a dosed character and is determined by the depth of paresis: the deeper the lesion, the longer the duration of treatment with the position (from 2-3 minutes to 1.5 hours).
Massage carried out differentially, in accordance with the localization of muscle damage. Weakened muscles are massaged more intensively; using the techniques of stroking and surface rubbing, their antagonists relax.
Physiotherapy treatment supplemented by electrical muscle stimulation.
The following method of therapeutic exercises gives a positive effect: active movements in the symmetrical joints of a healthy limb, passive movements in the joints of the affected limb, friendly active, lightweight exercises involving weakened muscles. Relief of the functional load is achieved by selecting the appropriate initial positions for performing exercises that reduce the inhibitory effect of the weight of the limb segment. To reduce friction, the limb segment is supported by a soft strap (on weight). Facilitate the work of paretic muscles and exercise in warm water. In the residual period, they continue to do therapeutic exercises; the number of applied exercises for training everyday and professional skills is significantly increased; game and sports-applied elements are introduced; optimal compensatory adaptations are formed.
The patient is prescribed massage(15-20 procedures). The massage course is repeated after 2-3 months.
Position treatment is determined by orthopedic tasks (sagging of the foot or hand) and is carried out with the help of orthopedic and prosthetic products (devices, splints, special shoes).
In this period, contractures and stiffness in the joints are of particular difficulty in treatment. The alternation of passive movements with active exercises of a different nature and massage of unaffected areas, thermal procedures allow you to restore the necessary range of motion.
With the persistence of secondary changes in tissues, apply mechanotherapy, which is effectively used in water.
Neuritis of the facial nerve
The most common causes of lesions of the facial nerve are infection, hypothermia, trauma, inflammatory diseases of the ear.
Clinical picture . It is mainly characterized by the acute development of paralysis or paresis of the facial muscles. The affected side becomes flabby, lethargic; blinking of the eyelids is disturbed, the eye does not completely close; the nasolabial fold is smoothed; the face is asymmetrical, drawn to the healthy side; speech is slurred; the patient cannot wrinkle his forehead, frown his eyebrows; loss of taste, lacrimation are noted.
Rehabilitation activities include positional therapy, massage, therapeutic exercises and physiotherapy.
Rehabilitation tasks:
Improving blood circulation in the face (especially on the side of the lesion), neck and the entire collar zone;
Restoration of the function of facial muscles, impaired speech;
Prevention of the development of contractures and friendly movements.
In the early period (1-10 days of illness), positional treatment, massage and therapeutic exercises are used. Treatment by position includes the following recommendations:
Sleep on your side (on the affected side);
For 10-15 minutes (3-4 times a day), sit with your head bowed in the direction of the lesion, supporting it with the back of the hand (supported by the elbow); pull the muscles from the healthy side to the side of the lesion (from bottom to top) with a handkerchief, while trying to restore the symmetry of the face.
To eliminate the asymmetry, adhesive plaster tension is applied from the healthy side to the patient, directed against the traction of the muscles of the healthy side. It is carried out by firmly fixing the free end of the patch to a special helmet-mask, made individually for each patient (Fig. 36).
Treatment position is carried out in the daytime. On the first day - 30-60 minutes (2-3 times a day), mainly during active facial actions (eating, talking). Then its duration is increased to 2-3 hours a day.
Massage start with the collar area and neck. This is followed by a facial massage. The patient sits down with a mirror in his hands, and the massage therapist is located opposite the patient in order to be sure to see his entire face. The patient performs the exercises recommended during the procedure, observing the accuracy of their execution with the help of a mirror. Massage techniques - stroking, rubbing, light kneading, vibration - are carried out according to a gentle technique. In the first days, the massage lasts 5-7 minutes; then its duration increases to 15-17 minutes.
Facial muscle massage is predominantly punctate, so that the skin displacements are insignificant and do not stretch the skin of the affected half of the face. The main massage is carried out from the inside of the mouth, and all massage movements are combined with therapeutic exercises.
Physiotherapy mainly addressed to the muscles of the healthy side - this is an isolated tension of the facial muscles and muscles surrounding the oral fissure. The duration of the lesson is 10-12 minutes (2 times a day).
In the main period (from the 10-12th day from the onset of the disease to 2-3 months), along with the use of massage and positional treatment, special physical exercises are performed.
Position treatment. Its duration increases to 4-6 hours a day; it alternates with LH and massage. The degree of tension of the adhesive plaster is also increased, reaching hypercorrection, with a significant shift to the diseased side, in order to achieve stretching and, as a result, weakening of the muscle strength on the healthy side of the face.
In some cases, adhesive plaster tension is carried out within 8-10 hours.
Exemplary special exercises for training mimic muscles
1. Raise your eyebrows up.
2. Wrinkle your eyebrows (frown).
3. Look down; then close your eyes, holding the eyelid on the side of the lesion with your fingers, and keep them closed for 1 minute; open and close your eyes 3 times in a row.
4. Smile with your mouth closed.
5. Squint.
6. Lower your head down, take a breath and, at the moment of exhalation, “snort” (vibrate your lips).
7. Whistle.
8. Flare the nostrils.
9. Raise the upper lip, exposing the upper teeth.
10. Lower the lower lip, exposing the lower teeth.
11. Smile with your mouth open.
12. Blow on a lit match.
13. Take water in your mouth, close your mouth and rinse, trying not to pour out the water.
14. Puff out your cheeks.
15. Move air from one half of the mouth to the other alternately.
16. Lower the corners of the mouth down (with the mouth closed).
17. Stick out the tongue and make it narrow.
18. Opening your mouth, move your tongue back and forth.
19. Opening your mouth, move your tongue left and right.
20. Pull out the lips with a "tube".
21. Follow with your eyes a finger moving in a circle.
22. Draw in the cheeks (with the mouth closed).
23. Lower the upper lip to the lower.
24. Use the tip of the tongue to drive along the gums alternately to the right and to the left (with the mouth closed), pressing the tongue against them with varying force.
Exercises to improve articulation
1. Pronounce the sounds "o", "and", "y".
2. Pronounce the sounds “p”, “f”, “v”, bringing the lower lip under the upper teeth.
3. Pronounce sound combinations: “oh”, “fu”, “fi”, etc.
4. Pronounce words containing these sound combinations by syllables (o-kosh-ko, Fek-la, i-zyum, pu-fik, Var-fo-lo-mei, i-vol-ga, etc.).
The listed exercises are performed in front of a mirror, with the participation of an exercise therapy instructor, and must be repeated by the patient on their own 2-3 times a day.
In the residual period (after 3 months), massage, positional treatment and therapeutic exercises are used, which are used in the main period. The proportion of therapeutic exercises, the task of which is the maximum possible restoration of facial symmetry, is significantly increasing. During this period, the training of facial muscles increases. Exercises for mimic muscles should be alternated with restorative and breathing exercises.
Brachial plexus neuritis
The most common causes of brachial plexus neuritis (plexitis) are: injury from dislocation of the humerus; wound; highly applied tourniquet for a long time. With the defeat of the entire brachial plexus, peripheral paralysis or paresis occurs and a sharp decrease in sensitivity in the arm.
Paralysis and atrophy of the following muscles develop: deltoid, biceps, internal shoulder, flexors of the hand and fingers (the arm hangs like a whip). In complex treatment, the leading method is position treatment: the brushes are given a half-bent position and laid on a splint with a roller placed in the area of the metacarpophalangeal joint.
The forearm and hand (in a splint) are hung on a scarf. Special exercises for the shoulder girdle, muscles of the shoulder, forearm and hand are recommended, as well as general developmental and breathing exercises.
A set of special exercises for plexitis (according to A.N. Tranquillitati, 1992)
1. I. p. - sitting or standing, hands on the belt. Raise your shoulders up - lower. Repeat 8-10 times.
2. I. p. - the same. Squeeze your shoulder blades, then return to the starting position. Repeat 8-10 times.
3. I.p. - the same, hands down. Raise your arms up (hands to your shoulders), spread your elbows to the sides, then press them back to your body. Circular movements of the arm bent at the elbow (movements in the shoulder joint) clockwise and against it. Repeat 6-8 times. The movements of the affected hand are performed with the help of an exercise therapy methodologist.
4. I.p. - too. Bend the injured arm, then straighten; take it to the side (straight or bent at the elbow), then return to the sp. Repeat 6-8 times. The exercise is performed with the help of a methodologist or a healthy hand.
5. I.p. - standing, leaning towards the injured arm (the other hand on the belt). Circular movements with a straight arm clockwise and against it. Repeat 6-8 times.
6. I.p. - too. Swing movements with both hands back and forth and crosswise in front of you. Repeat 6-8 times.
7. I.p. - standing or sitting. Leaning forward, bend the sore arm at the elbow and straighten it with the help of a healthy arm. Repeat 5-6 times.
8. I.p. - too. Turn the forearm and hand with the palm towards you and away from you. Repeat 6-8 times.
If necessary, movements are also performed in the wrist joint and finger joints.
Gradually, when the injured hand can already hold objects, exercises with a stick and a ball are included in the LG complex.
In parallel with therapeutic exercises, hydrocolonotherapy, massage and physiotherapy are prescribed.
Neuritis of the ulnar nerve
Most often, ulnar nerve neuritis develops as a result of nerve compression in the area of the elbow joint, which occurs in people whose work is associated with elbow support (on a machine, table, workbench), or when sitting for a long time, putting their hands on the armrests of a chair.
Clinical picture . The brush hangs down; no supination of the forearm; the function of the interosseous muscles of the hand is disturbed, in connection with which the fingers are claw-like bent ("clawed brush"); the patient cannot pick up and hold objects. There comes a rapid atrophy of the interosseous muscles of the fingers and the muscles of the palm from the side of the little finger; hyperextension of the main phalanges of the fingers, flexion of the middle and nail phalanges is noted; it is impossible to spread and adduct the fingers. In this position, the muscles that extensor the forearm are stretched, and contracture of the muscles that flex the hand occurs. Therefore, from the first hours of damage to the ulnar nerve, a special splint is applied to the hand and forearm. The hand is given a position of possible extension in the wrist joint, and the fingers are in a half-bent position; the forearm and hand are suspended on a scarf in the position of flexion at the elbow joint (at an angle of 80°), i.e. in the middle position.
Exercise therapy is prescribed on the 2nd day after the imposition of a fixing bandage. From the first days (due to the lack of active movements), passive gymnastics, gymnastics in water begin; doing a massage. As active movements appear, active gymnastics classes begin.
A.N. Tranquillitati proposes to include the following exercises in the complex of therapeutic exercises.
1. I.p. - sitting at the table; the arm, bent at the elbow, rests on it, the forearm is perpendicular to the table. Lowering the thumb down, raise the index finger up, then vice versa. Repeat 8-10 times.
2. I.p. - too. With a healthy hand, grab the main phalanges of the 2-5 fingers of the injured hand so that the thumb of the healthy hand is located on the side of the palm, and the others on the back of the hand. Bend and unbend the main phalanges of the fingers. Then, moving a healthy hand, also bend and unbend the middle phalanges.
Along with LH, electrical stimulation of the muscles innervated by the ulnar nerve is performed. When active movements appear, elements of occupational therapy (modeling from plasticine, clay), as well as learning to grasp small objects (matches, nails, peas, etc.) are included in the classes.
Neuritis of the femoral nerve
With neuritis of the femoral nerve, the quadriceps and tailor muscles are paralyzed. The movements of the patient with this disease are sharply limited: it is impossible to unbend the leg bent at the knee; (running and jumping are impossible; standing and climbing stairs are difficult, moving from a lying position to a sitting position. With neuritis of the femoral nerve, loss of sensitivity and acute pain are possible.
When muscle paralysis occurs, passive movements, massage are used. As the recovery progresses, active movements are used: leg extension, bringing the hip to the pelvis, moving from a lying position to a sitting position, exercises to overcome resistance (with blocks, springs, on simulators).
Along with therapeutic exercises, massage, electrical stimulation of paretic muscles, etc. are used.
Control questions and tasks
1. What symptoms are typical for the clinical picture of neuritis?
2. Tasks of complex restorative treatment of peripheral paralysis and characteristics of its periods.
3. Clinical picture of neuritis of the facial nerve and methods of rehabilitation in different periods.
4. Clinical picture of brachial plexus neuritis (plexitis). Special exercises for this disease.
5. Clinical picture of ulnar nerve neuritis. The method of exercise therapy for this disease.
Nervous system controls the activities of various organs and systems that make up the whole organism, communicates with the external environment, and also coordinates the processes occurring in the body depending on the state of the external and internal environment. It coordinates blood circulation, lymph flow, metabolic processes, which, in turn, affect the state and activity of the nervous system.
The human nervous system is conditionally divided into central and peripheral (Fig. 121). In all organs and tissues, nerve fibers form sensory and motor nerve endings. The first, or receptors, provide the perception of irritation from the external or internal environment and convert the energy of stimuli (mechanical, chemical, thermal, light, sound, etc.) in the process of excitation, which is transmitted to the central nervous system. Motor nerve endings transmit excitation from the nerve fiber to the innervated organ.
Rice. 121. Central and peripheral nervous system.
A: 1 - phrenic nerve;2 - brachial plexus;3 - intercostal nerves;4 - axillary nerve;5 - musculocutaneous nerve;6 - radial nerve;7 - median nerve;8 - ulnar nerve;9 - lumbar plexus;10 - sacral plexus;11 - pudendal and coccygeal plexus;12 - sciatic nerve;13 - peroneal nerve;14 - tibial nerve;15 - brain;16 - external cutaneous nerve of the thigh;17 - lateral dorsal cutaneous nerve;18 - tibial nerve.
B - segments of the spinal cord.
B - spinal cord:1 - white matter;2 - gray
substance;3 - spinal canal;4 - front horn;5 -
rear horn;6 - front roots;7 - back roots;8 -
spinal node;9 - spinal nerve.

G: 1 - spinal cord;2 - anterior branch of the spinal nerve;3 - posterior branch of the spinal nerve;4 - anterior root of the spinal nerve;5 - posterior root of the spinal nerve;6 - rear horn;7 - front horn;8 - spinal node;9 - spinal nerve;10 - motor nerve cell;11 - spinal node;12 - terminal thread;13 - muscle fibers;14 - sensitive nerve;15 - the end of the sensory nerve,16 - brain
It is known that higher motor centers are located in the so-called motor zone of the cerebral cortex - in the anterior central gyrus and adjacent areas. Nerve fibers from the indicated region of the cerebral cortex pass through the inner capsule, the subcortical regions and at the border of the brain and spinal cord make an incomplete decussation with the transition of most of them to the opposite side. Therefore, in diseases of the brain, motor disorders are observed on the opposite side: when the right hemisphere of the brain is damaged, the left half of the body is paralyzed, and vice versa. Further, the nerve fibers descend as part of the bundles of the spinal cord, approaching the motor cells, motoneurons of the anterior horns of the spinal cord. Motor neurons that regulate the movements of the upper limbs lie in the cervical thickening of the spinal cord (level V-VIII of the cervical and I-II thoracic segments), and the lower limbs - in the lumbar (level I-V of the lumbar and I-II sacral segments). The fibers coming from the nerve cells of the nuclei of the base nodes - the subcortical motor centers of the brain, from the reticular formation of the brain stem and cerebellum are also sent to the same spinal motor neurons. Thanks to this, the regulation of coordination of movements is ensured, involuntary (automated) movements are carried out and voluntary movements are prepared. The fibers of the motor cells of the anterior horns of the spinal cord, which are part of the nerve plexuses and peripheral nerves, end in the muscles (Fig. 122).

Rice. 122. Dermatome boundaries and segmental innervation(A, B), muscles
human(B), transverse section of the spinal cord(G).
A: C 1-8 - cervical;T 1-12 - chest;L1-5 - lumbar;S 1-5 - sacral.
B: 1 - cervical knot;2 - median cervical node;3 -
lower cervical node;4 - border sympathetic trunk;
5 - cerebral cone;6 - terminal (terminal) thread
meninges;7 - lower sacral node
sympathetic trunk.
B (front view):1 - frontal muscle;2 - chewing
muscle; 3 - sternocleidomastoid muscle;4 -
pectoralis major;5 - the latissimus dorsi muscle;6 -
serratus anterior;7 - white line;8 - seed
cord;9 - thumb flexor;10 -
quadriceps femoris;11 - long fibula
muscle;12 - anterior tibialis muscle;13 - long
extensor of fingers;14 - short muscles of the rear of the foot;15 -
facial muscles;16 - subcutaneous muscle of the neck;

17 - collarbone;18 - deltoid muscle;19 - sternum;20 - biceps muscle of the shoulder;21 - rectus abdominis;22 - muscles of the forearm;23 - umbilical ring;24 - worm-like muscles;25 - wide fascia of the thigh;26 - adductor muscle of the thigh;27 - tailor muscle;28 - extensor tendon retainer;29 - long extensor of the fingers;30 - external oblique muscle of the abdomen.
B (back view):1 - belt muscle of the head;2 - the latissimus dorsi muscle; 3 - ulnar extensor of the wrist;4 - extensor of the fingers;5 - muscles of the rear of the hand;6 - tendon helmet;7 - external occipital protrusion;8 - trapezius muscle;9 - spine of the scapula;10 - deltoid muscle;11 - rhomboid muscle;12 - triceps muscle of the shoulder;13 - medial epicondyle;14 - long radial extensor of the wrist;15 - chest-lumbar fascia;16 - gluteal muscles;17 - muscles of the palmar surface of the hand;18 - semimembranous muscle;19 - biceps;20 - calf muscle;21 - Achilles (heel) tendon
Any motor act occurs when an impulse is transmitted along the nerve fibers from the cerebral cortex to the anterior horns of the spinal cord and further to the muscles (see Fig. 220). In diseases (injuries of the spinal cord) of the nervous system, the conduction of nerve impulses becomes difficult, and a violation of the motor function of the muscles occurs. Complete loss of muscle function is called paralysis (plegia), and the partial paresis.
According to the prevalence of paralysis, there are: monoplegia(lack of movement in one limb - arm or leg), hemiplegia(damage to the upper and lower limbs of one side of the body: right-sided or left-sided hemiplegia), paraplegia(impaired movement in both lower limbs is called lower paraplegia, in the upper - upper paraplegia) and tetraplegia (paralysis of all four limbs). When peripheral nerves are damaged, paresis in the zone of their innervation, called the corresponding nerve (for example, paresis of the facial nerve, paresis of the radial nerve, etc.) (Fig. 123).
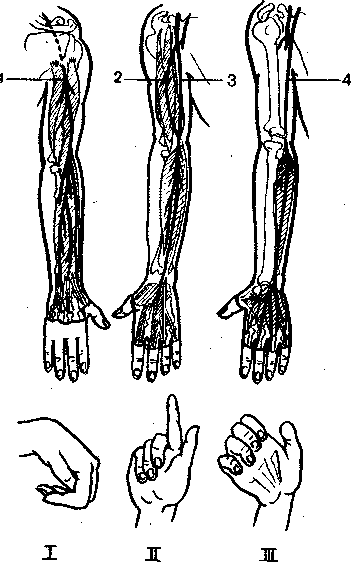
Rice. 123. Nerves of the upper limb;1 - radial nerve;2 - skin-
muscular nerve;3 - median nerve;4 - ulnar nerve.I - brush with damage to the radial nerve.II - brush with damage to the median nerve.III - hand with damage to the ulnar nerve
Depending on the localization of the lesion of the nervous system, peripheral or central paralysis (paresis) occurs.
With the defeat of the motor cells of the anterior horns of the spinal cord, as well as the fibers of these cells, which are part of the nerve plexuses and peripheral nerves, a picture of peripheral (flaccid), paralysis develops, which is characterized by a predominance of symptoms of neuromuscular prolapse: limitation or absence of voluntary movements, a decrease in muscle strength, decreased muscle tone (hypotension), tendon, periosteal and skin reflexes (hyporeflexia) or their complete absence. Often there is also a decrease in sensitivity and trophic disorders, in particular muscle atrophy.
To correctly determine the severity of paresis, and in cases of mild paresis - sometimes to identify it, it is important to quantify the state of individual motor functions: muscle tone and strength, and the volume of active movements. The available methods make it possible to compare and effectively control the results of rehabilitation treatment in a polyclinic and a hospital.
To study muscle tone, a tonometer is used, muscle strength is measured with a hand dynamometer, the volume of active movements is measured with a goniometer (in degrees).
In case of violation of the cortical-subcortical connections with the reticular formation of the brain stem or damage to the descending motor pathways in the spinal cord and, as a result, the function of the spinal motor neurons is activated as a result of a disease or brain injury, a syndrome of central spastic paralysis occurs. It, in contrast to peripheral and central "flaccid" paralysis, is characterized by an increase in tendon and periosteal reflexes (hyperflexia), the appearance of pathological reflexes, the occurrence of the same movements when trying to voluntarily act on a healthy or paralyzed limb (for example, abduction of the shoulder outward when bending the forearm of the paretic hands or clenching a paralyzed hand into a fist with a similar voluntary movement of a healthy hand).
One of the most important symptoms of central paralysis is a pronounced increase in muscle tone (muscle hypertension), which is why such paralysis is often called spastic. For most patients with central paralysis due to brain disease or injury, the Wernicke-Mann posture is characteristic: the shoulder is brought (pressed) to the body, the hand and forearm are bent, the hand is turned palm down, and the leg is extended at the hip and knee joints and bent at the foot. This reflects a predominant increase in the tone of the flexor and pronator muscles in the upper limb and extensor muscles in the lower.
With injuries and diseases of the nervous system, disorders occur that sharply reduce the efficiency of patients, often lead to the development of secondary paralytic deformities and contractures that adversely affect the musculoskeletal function. Common to all injuries and diseases of the nervous system are limitation of the range of motion, decreased muscle tone, vegetotrophic disorders, etc.
A deep understanding of the mechanisms of the pathology of the nervous system is the key to the success of rehabilitation measures. So, with discogenic sciatica, nerve fibers are infringed, causing pain, with a stroke, certain areas of motor nerve cells cease to function, so adaptation mechanisms play an important role.
In rehabilitation, compensatory-adaptive reactions of the body are important, which are characterized by the following common features: normal physiological functions of organs and tissues (their functions); adaptation of the organism to the environment, provided by the restructuring of vital activity due to the strengthening of some and the simultaneous weakening of other functions; they develop on a single, stereotyped material basis in the form of continuous variation in the intensity of renewal and hyperplasia of the cellular composition of tissues and intracellular structures; compensatory-adaptive reactions are often accompanied by the appearance of peculiar tissue (morphological) changes.
The development of regenerative processes in the nervous tissue occurs under the influence of preserved functions, that is, the nervous tissue is being restructured, the number of processes of nerve cells and their branches on the periphery changes; there is also a restructuring of synaptic connections and compensation after the death of part of the nerve cells.
The process of restoration of the nervous system occurs in nerve cells, nerve fibers and structural elements of tissues due to (or due to) restoration of membrane permeability and excitability, normalization of intracellular redox processes and activation of enzyme systems, which leads to the restoration of conductivity along nerve fibers and synapses.
The rehabilitation regimen should be adequate to the severity of the disease, which is assessed by the degree of impairment of adaptive activity. The level of damage to the central nervous system and peripheral nervous system is taken into account. Important factors are the ability to move independently, take care of oneself (perform housework, eat alone, etc.) and family, communicate with others, assess the adequacy of behavior, the ability to control physiological functions, as well as the effectiveness of training.
The complex rehabilitation system includes the use of exercise therapy, hydrokinesitherapy, various types of massage, occupational therapy, physiotherapy, spa treatment, etc. In each individual case, the combination and sequence of the use of certain rehabilitation means is determined.
In case of severe diseases (injuries) of the nervous system, rehabilitation is aimed at improving the general condition of patients, raising their emotional tone and shaping their correct attitude to the prescribed treatment and the environment: psychotherapy, symptomatic drug therapy, occupational therapy, music therapy, massage in combination with therapeutic exercises, etc. .
Exercise therapy in neurology has a number of rules, the observance of which makes this method the most effective: early use of exercise therapy; the use of its means and techniques to restore temporarily impaired functions or to maximize compensation for those lost; selection of special exercises in combination with general developmental, general strengthening exercises and massage; strict individuality of exercise therapy, depending on the diagnosis, age and gender of the patient; active and steady expansion of the motor mode from the lying position to the transition to the sitting position, standing, etc.
Special exercises can be conditionally divided into the following groups:
exercises that increase joint range of motion and muscle strength;
exercises aimed at restoring and improving coordination of movements;
antispastic and antirigid exercises;
ideomotor exercises (sending a mental impulse to a trained muscle group);
a group of exercises aimed at restoring or forming motor skills (standing, walking, manipulations with simple but important household objects: clothes, dishes, etc.);
passive exercises and exercises for stretching connective tissue formations, treatment with position, etc.
All of the above groups of exercises are combined in various combinations and depend on the nature and extent of the motor defect, the stage of rehabilitation, the age and gender of the patient.
Rehabilitation of neurological patients requires long-term training of compensatory mechanisms (walking on crutches, self-care, etc.) to ensure sufficient compensation for lost or impaired functions. However, at a certain stage (stages), the recovery process slows down, that is, stabilization occurs. The success of rehabilitation is different for a particular pathology. So, with osteochondrosis of the spine or lumbosacral sciatica, it is higher than with multiple sclerosis or vascular diseases.
Rehabilitation largely depends on the patient himself, on how diligently he performs the program prescribed by the rehabilitation doctor or exercise therapy methodologist, helps to correct it depending on his functional capabilities, and, finally, whether he continues recovery exercises after the rehabilitation period is over.
Brain injury (concussion)
All brain injuries are characterized by an increase in intracranial pressure, a violation of hemo- and liquor circulation, followed by a violation of cortical-subcortical neurodynamics with macro- and microscopic changes in the cellular elements of the brain. A concussion of the brain leads to headaches, dizziness, functional and persistent autonomic disorders.
In case of violations of motor functions for the prevention of contractures, exercise therapy is prescribed (passive, then passive-active movements, positional treatment, muscle stretching exercises, etc.), massage of the back and paralyzed limbs (first the legs are massaged, then the arms, starting from the proximal sections), and also affect the biologically active points (BAP) of the limbs.
With mild and moderate concussion, massage should be carried out from the second or third day after the injury in the patient's sitting position. First, the back of the head, neck, shoulder girdle are massaged, then the back to the lower corners of the shoulder blades, using stroking, rubbing, shallow kneading and light vibration. Finish the procedure by stroking from the scalp to the muscles of the shoulder girdle. The duration of the massage is 5-10 minutes. Course 8-10 procedures.
In the first 3-5 days, with mild and moderate concussion, cryomassage of the occipital region and muscles of the shoulder girdle is also used. The duration of the massage is 3-5 minutes. Course 8-10 procedures.
Injuries of the spine and spinal cord
Sometimes a spinal injury occurs in a position of hyperlordosis, and then a rupture of an intact intervertebral disc can occur.
The cervical spine is especially often injured when jumping into a shallow body of water, when, after hitting the head against the bottom, a traumatic prolapse of an intact intervertebral disc occurs, causing tritraplegia. Degenerative changes inevitably lead to herniation of the intervertebral discs, which in itself is not a cause for complaints, but due to trauma, a radicular syndrome occurs.
When the spinal cord is damaged, flaccid paralysis occurs, which is characterized by muscle atrophy, the impossibility of voluntary movements, the absence of reflexes, etc. Each muscle is innervated from several segments of the spinal cord (see Fig. 96), therefore, with damage or diseases, there may be not only paralysis, but also muscle paresis of varying severity, depending on the prevalence of lesions in the anterior horns of the gray matter of the spinal cord.
The clinical course of the disease depends on the degree of damage to the spinal cord and its roots (see Fig. 122). So, with injuries of the upper cervical spine, spastic tetraparesis of the extremities occurs. With lower cervical and upper thoracic localization (C 6 -T 4), flaccid paresis of the arms and spastic paresis of the legs occurs, with thoracic localization - paresis of the legs. With the defeat of the lower thoracic and lumbar segments of the spine, flaccid paralysis of the legs develops. The cause of flaccid paralysis can also be damage to the spinal cord with closed fractures of the spine and its injuries.
Prevention of the development of joint contractures by means of massage, exercise therapy, stretching exercises, physio- and hydrotherapy, hydrokinesitherapy is the main task for paralysis of any origin. In water, the possibility of active movements is facilitated and the fatigue of weakened muscles is reduced. Electrical stimulation of paralyzed muscles is carried out with needle electrodes with a preliminary introduction of ATP. In addition, positional treatment is included using staged plaster splints (bandages), teips, sandbags, etc., as well as staged redressing and other methods.
Timely use of the necessary rehabilitation means can completely prevent the development of contractures and other deformities.
Traumatic encephalopathy is a complex of morphological, neurological and mental disorders that occur in the late and long-term periods after a traumatic brain injury. Characterized by asthenic and various vegetative-vascular disorders, memory impairment by the type of retrograde amnesia, headaches, fatigue, irritability, sleep disturbance, heat intolerance, stuffiness, etc.
The recurrence of seizures indicates the development of traumatic epilepsy. In severe cases, traumatic dementia occurs with severe memory impairment, a decrease in the level of personality, etc.
In addition to dehydration therapy, complex treatment includes the use of anticonvulsants, tranquilizers, nootropics, etc. Massage, LH, walking, skiing help to improve the patient's well-being and prevent decompensation.
The massage technique includes massaging the collar area, back (to the lower corners of the shoulder blades), legs, as well as the effect on the BAP by the inhibitory or stimulating method, depending on the prevalence of one or another symptom. The duration of the massage is 10-15 minutes. Course 10-15 procedures. 2-3 courses per year. With a headache, cryomassage No. 5 is indicated.
Patients are not allowed to visit the bath (sauna), sunbathe, take hyperthermic baths!
Vascular epilepsy
The occurrence of epileptic seizures in dysciculatory encephalopathy is associated with the formation of cicatricial and cystic changes in the brain tissue and regional cerebral hypoxia.
The system of rehabilitation of patients includes exercise therapy: general developmental exercises, breathing, coordination. Exercises with straining, with weights, as well as with prolonged head tilts are excluded. Therapeutic exercises are performed at a slow pace, without sudden movements. Swimming, cycling, visiting the sauna (bath) are also excluded.
Physiotherapy includes electrosleep, drug electrophoresis No. 10, oxygen therapy. A general massage is performed, with the exception of percussion techniques. Occupational therapy is carried out on stands, box gluing, bookbinding, etc.
Osteocondritis of the spine
Degenerative changes in the intervertebral discs occur as a result of the physiological neuroendocrine aging process and due to wear and tear under the influence of one-time injuries or repeated microtraumas. Most often, osteochondrosis occurs in athletes, hammerers, typists, weavers, drivers, machine operators, etc.
General massage, cryomassage, vibration massage, LG (Fig. 124), hydrocolonotherapy help to restore the function of the spinal column as soon as possible. They cause deep hyperemia, improve blood and lymph flow, have an analgesic and resolving effect.
Massage technique. First, a preliminary back massage is performed using stroking techniques, shallow kneading of the muscles of the entire back. Then they proceed to massage the spinal column, using rubbing with the phalanges of four fingers, the base of the palm, kneading with the phalanges of the first fingers, forceps, ordinary and double ring kneading of the broad muscles of the back. Particularly carefully grind, knead BAP. Rubbing and kneading techniques should be alternated with stroking with both hands. In conclusion, active-passive movements are carried out, breathing exercises with an emphasis on exhalation and compression of the chest 6-8 times. The duration of the massage is 10-15 minutes. Course 15-20 procedures.
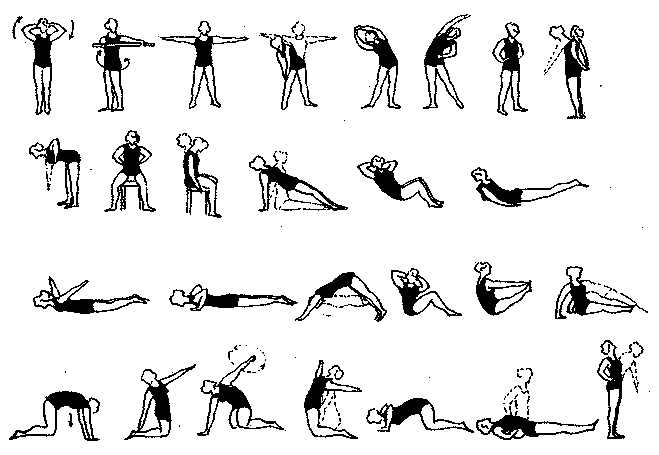
Rice. 124. Approximate complex of LH in osteochondrosis of the spine
Discogenic radiculitis
The disease often affects the intervertebral discs of the lower part of the spinal column. This is explained by the fact that the lumbar region has greater mobility and is subjected to the most intense static-dynamic loads on the muscular-ligamentous apparatus. Pain occurs when the spinal nerve roots are compressed by a disc herniation. The pain syndrome is characterized by acute development. Pain can occur in the morning, after heavy physical exertion, and in some cases is accompanied by muscle spasm. There is some limitation of movements in the lumbar spine, lumbar discomfort.
Conservative treatment is shown. Traction is carried out on the shield with a preliminary massage or heating with a solar lamp or manual therapy. After the disappearance of pain - LH in the prone position, on all fours, in the knee-elbow position. The pace is slow to avoid pain. Exercises with inclinations in a standing position are excluded.
Massage objectives: to provide analgesic and anti-inflammatory effects, to promote the speedy recovery of spinal function.
Massage technique. First, stroking, light vibration is performed in order to relieve tension in muscle tone, then longitudinal and transverse kneading of the broad muscles of the back, rubbing with fingertips along the spinal column. Tapping, chopping should not be used to avoid muscle spasm and increased pain. After the procedure, traction is carried out on a shield or in water. The duration of the massage is 8-10 minutes. Course 15-20 procedures.
lumbosacral pain spinal injuries occur, as a rule, immediately after a fall, blow, etc. In mild cases, transient lumbodynia develops with pain in the lumbar region. Acute pain can result from excessive flexion in the lumbosacral region.
LH is performed in the supine position. Includes exercises to stretch the sciatic nerve. Raising the legs up 5-8 times; "bicycle" 15-30 s; turns of the legs bent at the knee and hip joints to the left and to the right 8-12 times; raise the pelvis, pause for a count of 5-8, then return to the starting position. The last exercise is diaphragmatic breathing.
Massage objectives: to provide analgesic and anti-inflammatory effects, improve blood and lymph flow in the damaged area.
Massage technique. The initial position of the patient is lying on his stomach, a roller is placed under the ankle joints. Planar and embracing stroking is applied with the palms of both hands. Kneading is performed with both hands both longitudinally and transversely, while massage movements are performed in ascending and descending directions. In addition, planar stroking is used with the first fingers of both hands in the upward direction, rubbing and kneading with the fingertips, the base of the palm along the spinal column. All massage techniques should be alternated with stroking. Do not use chopping, tapping and intensive kneading. In the early days, the massage should be gentle. The duration of the massage is 8-10 minutes. Course 15-20 procedures.
Lumbago (lumbago) is perhaps the most common manifestation of pain in the lumbar region. Attack-like developing acute piercing pains are localized in the muscles of the lower back and lumbo-dorsal fascia. The disease often occurs in people engaged in physical labor, in athletes, etc., with the combined effect of tension in the lumbar muscles and hypothermia. Chronic infections also play an important role. Pain usually lasts for several days, sometimes 2-3 weeks. Pathophysiologically, with lumbago, there is a tear of the muscle bundles and tendons, hemorrhages in the muscles, and the subsequent phenomena of fibromyositis.
LH (general developmental exercises, stretching exercises and breathing exercises) are performed in the prone position and knee-elbow. The pace is slow. Traction on the shield and cupping massage are shown.
Massage technique. First, a preliminary massage of all the muscles of the back is carried out, then stroking, rubbing and shallow kneading of the muscles of the lumbar region. Professor S.A. Flerov recommends massaging the lower hypogastric sympathetic plexus in the lower abdomen, at the site of bufurcation of the abdominal aorta. Observations show that massage according to the method of S.A. Flerova relieves pain. In the acute period, cryomassage No. 3 is indicated.
sciatica
According to most authors, the disease is caused mainly by congenital or acquired changes in the spinal column and its ligamentous apparatus. Significant and prolonged physical stress, trauma, unfavorable microclimatic conditions, and infections contribute to the development of the disease.
The pain of sciatica can be sharp or dull. It is localized in the lumbosacral region, usually on one side, radiates to the buttock, back of the thigh, outer surface of the lower leg, sometimes combined with numbness, paresthesia. Hyperesthesia is often found
Therapeutic exercise in diseases of the nervous system plays a significant role in the rehabilitation of neurological patients. Treatment of the nervous system is impossible without therapeutic exercises. Exercise therapy for diseases of the nervous system has the main goal of restoring self-care skills and, if possible, complete rehabilitation.
It is important not to miss the time to create the correct new motor stereotypes: the earlier treatment is started, the easier, better and faster the compensatory-adaptive recovery of the nervous system occurs.
In the nervous tissue, the number of processes of nerve cells and their branches on the periphery increases, other nerve cells are activated, and new nerve connections appear to restore lost functions. Timely adequate training is important for creating the correct stereotypes of movements. So, for example, in the absence of physiotherapy exercises, a "right-brained" stroke patient - a restless fidget "learns" to walk, pulling the paralyzed left leg to the right and dragging it behind him, instead of learning to walk correctly, with each step moving the leg forward and then transferring the center of gravity of the body to it. If this happens, then it will be very difficult to retrain.
Not all patients with diseases of the nervous system can do the exercises on their own. Therefore, they cannot do without the help of their relatives. To begin with, before starting therapeutic exercises with a patient who has paresis or paralysis, relatives should master some techniques for moving the patient: transplanting from bed to chair, pulling up in bed, walking training and so on. In fact, this is a safety technique to prevent excessive stress on the spine and joints of the caregiver. Lifting a person is very difficult, so all manipulations must be performed at the level of a magician in the form of a “circus trick”. Knowing some special techniques will greatly facilitate the process of caring for the sick and help maintain your own health.
Features of exercise therapy in diseases of the nervous system.
one). Early initiation of exercise therapy.
2). Adequacy of physical activity: physical activity is selected individually with a gradual increase and complication of tasks. A slight complication of the exercises psychologically makes the previous tasks “easy”: what previously seemed difficult, after new slightly more complex tasks, is performed more easily, with high quality, the lost movements gradually appear. It is impossible to allow overload in order to avoid deterioration of the patient's condition: motor disturbances may increase. In order for progress to occur faster, it is necessary to finish the lesson on the exercise that this patient has, to focus on this. I attach great importance to the psychological preparation of the patient for the next task. It looks something like this: "Tomorrow we will learn to get up (walk)." The patient thinks about it all the time, there is a general mobilization of forces and a readiness for new exercises.
3). Simple exercises are combined with complex ones for training higher nervous activity.
4). The motor mode gradually steadily expands: lying - sitting - standing.
Therapeutic exercise for diseases of the nervous system.5). All means and methods of exercise therapy are used: therapeutic exercises, positional treatment, massage, extension therapy (mechanical straightening or stretching along the longitudinal axis of those parts of the human body that have a disturbed anatomical location (contractures)).
The main method of physical therapy for diseases of the nervous system is therapeutic exercises, the main means of exercise therapy are exercises.
Apply
Isometric exercises aimed at strengthening muscle strength;
- exercises with alternating tension and relaxation of muscle groups;
- exercises with acceleration and deceleration;
- coordination exercises;
- balance exercise;
- reflex exercises;
- ideomotor exercises (with mental sending of impulses). It is these exercises that I use for diseases of the nervous system - - - - most often in combination with Su-jok therapy.
Damage to the nervous system occurs at different levels, the neurological clinic depends on this and, accordingly, the selection of therapeutic exercises and other physiotherapeutic therapeutic measures in the complex treatment of a particular neurological patient.
Hydrokinesitherapy - exercises in water - a very effective method of restoring motor functions.
Exercise therapy for diseases of the nervous system is divided according to the parts of the human nervous system, depending on which part of the nervous system is affected:
exercise therapy for diseases of the central nervous system;
exercise therapy for diseases of the peripheral nervous system;
exercise therapy for diseases of the somatic nervous system;
Exercise therapy for diseases of the autonomic nervous system.
Some subtleties of work with neurological patients.
In order to calculate our strength in caring for a neurological patient, we will consider some significant factors, since the care process is complex, and it is not always possible to cope alone.
The state of mental activity of a neurological patient.
The patient's experience in physical education before illness.
The presence of excess weight.
Depth of damage to the nervous system.
Accompanying illnesses.
For physiotherapy exercises, the state of higher nervous activity of a neurological patient is of great importance: the ability to be aware of what is happening, to understand the task, to concentrate attention when performing exercises; volitional activity plays a role, the ability to resolutely tune in to daily painstaking work in order to achieve the goal of restoring the body's lost functions.
In the case of a stroke or brain injury, most often the patient partially loses the adequacy of perception and behavior. Figuratively, it can be compared with the state of a drunk person. There is a "disinhibition" of speech and behavior: the shortcomings of character, upbringing and inclination to what is "impossible" are exacerbated. Each patient has a behavioral disorder that manifests itself individually and depends on the
one). what activity the patient was engaged in before the stroke or before the brain injury: mental or physical labor (it is much easier to work with intellectuals if the body weight is normal);
2). how developed the intellect was before the disease (the more developed the intellect of a patient with a stroke, the more the ability to purposefully exercise exercise remains);
3). in which hemisphere of the brain did the stroke occur? "Right hemispheric" stroke patients behave actively, show emotions violently, do not hesitate to "express"; they do not want to follow the instructions of the instructor, they start walking ahead of time, as a result, they have a risk of forming incorrect motor stereotypes. “Left hemispheric” patients, on the contrary, behave inactively, do not show interest in what is happening, just lie down and do not want to engage in physiotherapy exercises. It is easier to work with "right hemisphere" patients, it is enough to find an approach to them; what is needed is patience, a delicate and respectful attitude, and the decisiveness of methodological instructions at the level of a military general. :)
During classes, instructions should be given decisively, confidently, calmly, in short phrases, it is possible to repeat instructions due to the patient's slow perception of any information.
In case of loss of behavioral adequacy in a neurological patient, I have always effectively used the “cunning”: you need to talk to such a patient as if he is a completely normal person, not paying attention to “insults” and other manifestations of “negativity” (unwillingness to engage in, denial of treatment other). It is not necessary to be verbose, it is necessary to make small pauses so that the patient has time to realize the information.
In case of damage to the peripheral nervous system, flaccid paralysis or paresis develops. If at the same time there is no encephalopathy, then the patient is capable of much: he can independently exercise a little during the day several times, which undoubtedly increases the chance of restoring movements in the limb. Flaccid paresis is more difficult to respond to than spastic paresis.
* Paralysis (plegia) - the complete absence of voluntary movements in the limb, paresis - incomplete paralysis, weakening or partial loss of movement in the limb.
It is necessary to take into account another important factor: whether the patient was engaged in physical education before the disease. If physical exercises were not included in his lifestyle, then rehabilitation in case of a disease of the nervous system becomes much more complicated. If this patient has exercised regularly, then the recovery of the nervous system will be easier and faster. Physical labor at work does not belong to physical education and does not bring benefits to the body, since it is the exploitation of one's own body as a tool for doing work; he does not add health due to the lack of dosing of physical activity and control of well-being. Physical labor is usually monotonous, so there is wear and tear of the body in accordance with the profession. (So, for example, a painter-plasterer "earns" humeroscapular periarthrosis, a loader - osteochondrosis of the spine, a massage therapist - osteochondrosis of the cervical spine, varicose veins of the lower extremities and flat feet, and so on).
For home exercise therapy for diseases of the nervous system, you will need ingenuity to select and gradually complicate exercises, patience, regularity of daily exercises several times during the day. It will be much better if in the family the burden of caring for the sick is distributed to all family members. The house should be in order, cleanliness and fresh air.
It is desirable to put the bed so that it has access from the right and left sides. It should be wide enough to allow the patient to be rolled from side to side when changing bed linen and changing body position. If the bed is narrow, then each time you have to pull the patient to the center of the bed so that he does not fall. Additional pillows and rollers will be needed to create a physiological position of the limbs in the supine position and on the back, a splint for the paralyzed arm to prevent contracture of the flexor muscles, a regular chair with a back, a large mirror so that the patient can see and control his movements (especially the mirror necessary in the treatment of neuritis of the facial nerve).
There should be room on the floor for lying down exercises. Sometimes you need to make handrails for support with your hands in the toilet, in the bathroom, in the corridor. To do therapeutic gymnastics with a neurological patient, you will need a wall bar, a gymnastic stick, elastic bandages, balls of different sizes, skittles, a roller foot massager, chairs of different heights, a step bench for fitness and much more.






")


- What was taught to women who became guards in concentration camps Torture used by the Nazis
- Singer Alex Malinovsky: biography, career, personal life, photo Let's start the story again
- Do I need to shave the testicles and how to do it right at home How to shave the eggs
- Chinese girls with small breasts
- Famous girls with small breasts
- Shoulder girdle: why you can’t sympathize with Russian truckers
- How to clean your computer from junk and speed up its work
- Wedding predictions for guests: funny and funny ideas Comic fortune-telling of a gypsy in prose
- Business on coffee grounds or how to open a mobile coffee shop on wheels?
- Congratulation of a gypsy on a woman's anniversary
- Define the concepts: choir, vocal ensemble, trio, duet, solo
- Guy's Room Design: Ideas and Examples
- General rules for drawing up a foundation plan House foundation drawings
- modern art deco bedroom small art deco bedroom
- Pansies: characteristics and photos of flowers
- Making an art deco bedroom: the choice of materials Beige art deco bedroom
- Bedroom interiors in art deco style Bedroom art deco style beige
- Young: planting and care in the open field Young planting and care in the open
- Varieties for open ground
- Pansies: cultivation and care in the open field