Bones forming the wrist joint. The wrist joint is a perfect motor apparatus of the upper limb. Bruise and compression
Some joints of the human musculoskeletal system are completely unremarkable in appearance, although they have a rather complex internal structure. These joints include the wrist joint, which anatomically and functionally connects two sections of the upper limb - the forearm and hand. Thanks to its stabilizing function, people can perform such a huge range of precise movements.
In fact, given the anatomy of mammals (which includes humans), the wrist joint should be similar in structure to the ankle joint. But evolution ensured its significant transformation, which was caused by the need to perform certain movements with the hands. Therefore, functional and anatomical changes occurred in it almost in parallel, adapting the articulation to the needs of the body.
But the wrist joint is interesting not only because of the complex anatomy of the bones - the structure of the soft tissues is also of interest. From the outside, it is enveloped by an interweaving of many structures - vessels and nerves. They all go to the brush, which requires a huge number of feeding and holding elements to work accurately. Therefore, the wrist joint must not only have good mobility, but also ensure the safety of all these formations.
General anatomy
Before moving on to a description of the individual elements of the connection, we should dwell on its anatomical characteristics. All musculoskeletal systems are divided into several groups according to the general classification. This allows you to combine them together according to similar characteristics for ease of study:
- First of all, you should decide on the location - the wrist joint belongs to the joints of the upper limb. More precisely, it is located in the distal group, that is, it is located furthest from the body.
- Judging by the number of bones included in its composition, it can without hesitation be classified as a complex compound. In total, it has five articular surfaces - four of them are formed by bones, and one is formed by a triangular cartilaginous plate.
- The shape of the joint is ellipsoidal - the articular surface of the bones on each side is an elongated circle. This structure does not give it a good supporting function, but it does provide significant mobility.
Although the wrist joint consists of five elements, during movement and at rest it is a single structure, the parts of which are closely connected to each other by means of ligaments.
Bones of the forearm
Contrary to misconceptions, on the side of the forearm, only one articular bone surface is involved in the formation of the wrist joint. The ulna in its final section forms a head, which connects to the radius in the form of a low-moving distal radioulnar joint. Therefore, on the side of the forearm, the joint is formed a little unusually:
- Closer to the wrist, the radius bone turns into a massive thickening, which bears a significant part of the load during movements. The outer and central sections of the joint are formed by its wide articular surface. It is not perfectly smooth, having a depression in the central part. This shape ensures reliable fixation of the wrist bones, preventing them from moving excessively.
- The internal part of the human joint is formed by a triangular cartilaginous plate, which is located inside its cavity. It has a relatively mobile connection with the radius and ulna through ligaments. In general, this plate plays the role of a meniscus, providing improved contact between the articular surfaces.
A feature of the wrist joint is the unusual ratio between the number of bones - on the side of the forearm there is only one, although from the wrist it includes three formations at once.
Carpal bones

This section, anatomically the beginning, is formed from many small bone structures interconnected by strong ligaments. Although the wrist is considered a relatively unified structure, it still experiences a small range of motion when moving. The wrist joint includes only the lower row, directly adjacent to the radius:
- Coming from the thumb, the first structure is the scaphoid bone. It is distinguished by its curved shape, as well as its largest dimensions, adjacent to almost 50% of the articular surface on the side of the forearm.
- The central position is occupied by the lunate bone, the external structure of which fully corresponds to its name. On the lower surface it has a notch covered with articular cartilage. This formation connects it with the opposite side.
- The triquetral bone looks like a pyramid, the top of which is directed towards the forearm. It has an articular surface in the shape of a circle, with which it is adjacent to the outer part of the joint - in the area of the triangular cartilaginous disc.
The connection of all of these bones with each other also allows us to expand the boundaries and distinguish the complex and combined carpal joint - a set of joints of the wrist and radiocarpal joint.
Soft fabrics

Given the large number of bone structures, the joint capsule in humans should also differ in significant size. But the anatomy of the wrist joint is rich in features, so the shell is attached only along the very edge of the bones that form it. You can briefly describe its boundaries:
- From below, the capsule almost at the same level bends around the articular circumference of the radius, anchoring literally a few millimeters from its edge. Only on the inner surface the shell extends a little further - to the styloid process of the ulna, covering the cartilaginous disc.
- From above, the capsule, despite the presence of three separate articular surfaces, does not form any partitions or adhesions. It runs exactly along the edge of the scaphoid, lunate and triquetrum bones, enclosing them in a single cavity.
This structure is due to the large number of tendons, vessels and nerves surrounding the joint, for which an overdeveloped capsule would be a serious mechanical obstacle.
Ligaments
To ensure reliable performance of supporting and dynamic functions, such a complex joint requires a large number of supporting elements. Their role is played by their own ligaments, which not only hold the articular surfaces, but also fasten the individual bones of the wrist together. In general, five such formations can be distinguished:
- The lateral radial ligament of the wrist connects the styloid process of the bone structure of the same name with the outer edge of the scaphoid bone. When tensioned, it limits excessive outward movement of the hand - adduction.
- The lateral ulnar ligament of the wrist is located on the opposite side, connecting the ulnar and triquetral bones. Its purpose is to prevent strong deviation of the hand during inward movements.
- On the dorsal surface of the joint there is the widest and most powerful tendon, almost completely covering the joint - the dorsal radiocarpal ligament. It starts from just above the radial articular circumference, after which its fibers diverge towards the bones of the wrist. Its task is to limit excessive flexion of the wrist.
- The volar radiocarpal ligament is much smaller - it arises from the radial styloid process and runs towards the wrist. When it is stretched, the extension of the palm is limited.
- Individual fibers of the interosseous ligaments are also released, which connect all the bones of the wrist, making them practically immobile.
The listed structures are often damaged as a result of injury, which causes various mobility impairments in the joint.
Channels

Directly adjacent to the palmar surface of the wrist joint are special formations - the carpal canals, in which tendons, vessels and nerves pass. They allow you to divide them into separate bundles to avoid mechanical impact on them during movements:
- The ulnar canal occupies the innermost position, located between the ulnar bone and the broad ligament. It contains the ulnar nerve, which innervates the palm in the direction of the fourth and fifth fingers, as well as a vascular bundle, including an artery and veins.
- The radial canal passes between the bone with the same name and the same broad ligament. It contains only two anatomical structures - the carpal flexor tendon and the radial artery, which extends to the base of the thumb.
- The central carpal tunnel is the most saturated - it is bisected by synovial sheaths for the digital flexors. In addition to them, the median nerve passes there, as well as the accompanying artery.
Carpal tunnel syndrome is often observed, a pathology associated with mechanical pressure on nerve fibers (usually the median nerve).
Blood supply

The joint is nourished mainly by the extensive vascular network of the palm, from which individual branches extend to the joint. The outflow of blood occurs according to the same principle - the veins accompany the arteries:
- The blood supply to the joint comes from three sources - the main vessels of the forearm - the radial, ulnar and interosseous arteries. In the area of the transition to the palm, they form many connections - anastomoses, forming a branched network. From it, separate vessels extend to the back and palmar surface of the joint to its shell, delivering nutrients and oxygen.
- The outflow of blood is carried out into the system of deep veins of the forearm with similar names, only having a paired number. Also, many small veins form on the dorsal and palmar surface, which then flow into the common deep venous arch of the wrist.
A large number of sources of blood supply ensures good nutrition of the joint, and therefore its excellent ability to recover.
Innervation

The only significant formation with a large number of nerve endings is the joint capsule. There are different types of receptors on it - providing a feeling of pressure, pain or stretching. This feature makes it possible to prevent excessive stretching of the membrane by promptly engaging the muscles in work using reflex stimuli.
The source of all nerve fibers in the area of the wrist joint is the brachial plexus, which ensures the functioning of the entire upper limb. Three of its branches participate in the innervation of the joint capsule:
- The ulnar nerve passes through the canal in the area of the internal styloid process, heading to the area of the eminence of the little finger on the palm. On the wrist, small branches extend from it, innervating a small part of the membrane.
- The median nerve is located in the central canal, from which it supplies some fibers for the joint capsule. Due to them, the sensitivity of the entire front surface of the joint is ensured.
- The radial nerve runs along the dorsum of the forearm, going to the same side of the palm. In the area of the thumb, it also directs branches to the joint membrane, providing innervation to its entire posterior half.
If any of the nerve fibers are damaged, the functioning of the joint capsule also deteriorates, which leads to disruption of its recovery processes.
Physiology of movements

The ellipsoidal shape of the joint implies the implementation of movements in it that take place along two different axes. But in practice, it turns out that in the wrist joint mobility occurs in three directions at once. This feature is due to its joint work with the forearm joints - distal and proximal radioulnar.
The need for combined work is dictated by the purpose of the upper limb - to perform precise and targeted movements. Therefore, the initially biaxial joint additionally acquired another useful function:
- The main job that the articulation performs thousands of times every day is mobility in the frontal axis. In this case, coordinated contractions of the muscles of the anterior or posterior group of the forearm occur - the flexors or extensors of the wrist. With the help of tendons, they provide flexion or extension of the hand.
- Auxiliary movements are movements in the sagittal axis - drawn perpendicular to the palm. More complex mechanisms are responsible for their implementation - mainly the muscles on the inner or outer surface of the forearm contract. The result of such coordinated work is abduction or adduction—deviation of the hand outward or inward.
- Combined is the movement of the palm along the vertical axis, which is carried out with the help of other joints of the forearm. Contraction of the pronator or supinator muscles ensures the activation of this mechanism. In this case, there is a simultaneous rotation of the palm together with the forearm outward or inward.
Currently, combined mobility in the carpal joint is also being considered. It is assumed that during movements in the wrist joint, the joints of the wrist also experience some displacement, which is not noticeable only externally.
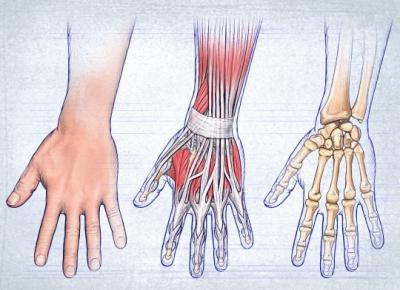
Upon careful examination, the structure, like any other part of our musculoskeletal system, is quite complex. It consists of three main structures: bones, muscles and ligaments that hold the bones. The hand has three sections, namely the wrist, fingers and metacarpus.
In this article we will take a closer look at the hand: the joints of the hand. Let's start with a description of the bones in its different sections.
Carpal bones
Since the hands must perform fairly precise and intricate movements, the structure of the bones of the hand is also extremely complex. The wrist has 8 small, irregularly shaped bones arranged in two rows. In the figure below you can see the structure of the right hand.
The proximal row forms an articular surface convex to the radius. It includes bones, counting from the fifth toe to the thumb: pisiform, triquetrum, lunate and scaphoid. The next row is distal. It connects to an irregularly shaped proximal joint. The distal row consists of four bones: trapezoid, polygonal, capitate and hamate.
Metacarpal bones
This section, consisting of 5 tubular parts, also demonstrates the intricate structure of the hand. The skeleton of these tubular bones is complex. Each of them has a body, a base and a head. The 1st finger is shorter than the others and is massive. The second metacarpal bone is the longest. The rest decrease in length as they move away from the first and approach the ulnar edge. The bases of the aforementioned metacarpal bones articulate with the bones that form the carpus. The first and fifth metacarpal bones have bases with saddle-shaped articular surfaces, the others are flat. The heads of the metacarpal bones, having an articular surface (hemispherical), articulate with the proximal digital phalanges.
Finger bones

Each finger, with the exception of the first, which consists of only two phalanges and does not have a middle one, has 3 phalanges: distal, proximal and middle (intermediate). The shortest are distal; proximal - the longest. At the distal end there is the head of the phalanx, and at the proximal end there is its base.
Sesamoid bones of the hand
In the thickness of the tendons, in addition to the indicated bones, there are sesamoids, located between the proximal phalanx of the thumb and its metacarpal bone. There are also unstable sesamoid bones. They are located between the proximal phalanges of the fifth and second fingers and their metacarpal bones. Typically, the sesamoid bones are located on the palmar surface. But sometimes they can be found on the back. The pisiform bone also belongs to the above-mentioned species. The sesamoid bones and their processes increase the leverage of the muscles attached to them.
We have examined the structure of the hand and bones of the hand, now we move on to the ligamentous apparatus.
Wrist joint
It consists of the radius and the bones of the proximal row of the wrist: triquetrum, lunate and scaphoid. The ulna is complemented by an articular disc and does not reach the wrist joint. The main role in the formation of the elbow joint is played by the radius. The wrist joint is elliptical in shape. It allows abduction, adduction, flexion and extension of the hand. A small passive rotational movement (10-12 degrees) is also possible in this joint, but is carried out due to the elasticity of the articular cartilage. Through the soft tissues it is easy to detect the gap of the wrist joint, which can be palpated from the ulnar and radial sides. From the ulna you can feel the depression between the triquetral bone and the head of the ulna. On the radial side there is a gap between the scaphoid bone and the lateral styloid process.
The movements of the wrist joint are closely related to the work of the midcarpal joint, located between the distal and proximal rows. Its surface is complex and irregular in shape. When flexing and extending, the range of mobility reaches 85 degrees. The adduction of the hand in the above-mentioned joint reaches 40 degrees, abduction - 20. The wrist joint can perform circumduction, i.e. Roundabout Circulation.
This joint is strengthened by numerous ligaments. They are located between individual bones, as well as on the lateral, medial, dorsal and palmar surfaces of the wrist. (radial and ulnar) play the most important role. On the ulnar and radial sides, between the bony elevations, there is a flexor retinaculum - a special ligament. In fact, it does not belong to the joints of the hand, being a thickening of the fascia. The flexor retinaculum turns the carpal groove into a canal for the median nerve and digital flexor tendons. Let us continue to describe the anatomical structure of the hand.
Carpometacarpal joints
They are flat in shape and inactive. The exception is the thumb joint. The range of motion of the carpometacarpal joints is no more than 5-10 degrees. They have limited mobility because the ligaments are well developed. Located on the palmar surface, they form a stable palmar ligamentous apparatus that connects the bones of the wrist and metacarpals. There are arcuate ligaments on the hand, as well as transverse and radial ones. The capitate bone is central to the ligamentous apparatus, and the ligaments are attached to it. The palmar ones are much better developed than the dorsal ones. The dorsal ligaments connect the bones of the wrist. They form thickening capsules that cover the joints located between these bones. The interosseous are located in the second row of carpal bones.
In the thumb, the carpometacarpal joint is formed by the base of the first metacarpal and polygonal bone. The articular surfaces are saddle-shaped. This joint can perform the following actions: abduction, adduction, reposition (backward movement), opposition (opposition) and circumduction (circular movement). The volume of grasping movements, due to the fact that the thumb is opposed to all the others, increases significantly. The mobility of the carpometacarpal joint of this finger during adduction and abduction is 45-60 degrees, and 35-40 during reverse movement and opposition.

Structure of the hand: metacarpophalangeal joints
These joints of the hand are formed by the heads of the metacarpal bones with the participation of the bases of the proximal phalanges of the fingers. They are spherical in shape, have 3 axes of rotation perpendicular to each other, around which extension and flexion, abduction and adduction, as well as circular movements (circumduction) are carried out. Adduction and abduction are possible by 45-50 degrees, and flexion and extension by 90-100. These joints have collateral ligaments located on the sides that strengthen them. Palmar, or accessory, are located on the palmar side of the capsule. Their fibers are intertwined with the fibers of the deep transverse ligament, which prevents the heads of the metacarpal bones from diverging in different directions.
Interphalangeal joints of the hand
They are block-shaped, and their axes of rotation run transversely. Extension and flexion are possible around these axes. The proximal interphalangeal joints have a range of flexion and extension equal to 110-120 degrees, distal ones - 80-90. The interphalangeal joints are very well strengthened thanks to the collateral ligaments.
Synovial and fibrous sheaths of the tendons of the fingers
The extensor retinaculum, like the flexor retinaculum, plays a huge role in strengthening the position of the tendons of the muscles running underneath them. This is especially true when working with the hand: when extending and bending it. Nature has conceived a very competent structure that finds support in the above-mentioned ligaments from their inner surface. Separation of tendons from bones is prevented by ties. This allows you to withstand high pressure during intense work and strong muscle contraction.
Special tendon sheaths, which are bone-fibrous or fibrous canals, help reduce friction and slip of the tendons running to the hand from the forearm. They contain synovial vaginas. The largest number of them (6-7) is located under the extensor retinaculum. The radius and ulna have grooves that correspond to the location of muscle tendons. And also the so-called fibrous bridges, which separate the canals from each other and pass to the bones from the extensor retinaculum.

Palmar synovial sheaths belong to the flexor tendons of the fingers and hands. The common synovial sheath extends to the center of the palm and reaches the distal phalanx of the fifth finger. The tendons of the superficial and deep digital flexors are located here. The thumb has a long flexor tendon, located separately in the synovial sheath and passing onto the finger along with the tendon. The synovial sheaths in the palm area lack the tendons of the muscles that go to the fourth, second and third fingers. Only the tendon of the fifth finger has a synovial sheath, which is a continuation of the common one.
Muscles of the hand
In the picture below you can see the muscles of the arm. The structure of the hand is shown here in more detail.

There are muscles in the hand only on the palmar side. They are divided into three groups: middle, thumb and small fingers.
Since finger movements require great precision, there are a significant number of short muscles in the hand, which complicate the structure of the hand. We will consider the arm muscles of each group below.
Middle muscle group
It is formed by worm-shaped muscles, starting from the tendons of the deep flexor of the fingers and attached to the proximal phalanges, or rather their bases, from the second to the fifth finger, if we consider the structure of the hand. These hand muscles also come from the dorsal and palmar interosseous muscles, located in the spaces between the bones of the metacarpus, attached to the base of the proximal phalanges. The function of this group is that these muscles are involved in flexing the proximal phalanges of the named fingers. Thanks to the palmar interosseous muscles, it is possible to bring the fingers to the middle finger of the hand. With the help of the dorsal interosseous, they are pulled apart.
Muscles of the thumb

This group forms the eminence of the thumb. These muscles begin near the nearby bones of the metacarpus and wrist. As for the thumb, its flexor brevis inserts near the sesamoid bone, which is located near the base of the proximal phalanx. The adductor pollicis muscle goes to the first bone of the metacarpus, and the adductor pollicis muscle is located on the side of the internal sesamoid bone.
Muscles of the small finger
This group of muscles forms an elevation on the inside of the palm. These include: the abductor digiti minimi, the opponens minimi, the palmaris brevis, and the flexor brevis muscle.
They originate from nearby bones in the wrist. These muscles are attached to the base of the fifth finger, more precisely its proximal phalanx, and to the fifth metacarpal bone. Their function is reflected in the name.
In the article we tried to most accurately represent the structure of the hand. Anatomy is a fundamental science that, of course, requires more careful study. Therefore, some questions remained unanswered. The structure of the hand and wrist is a topic that interests not only doctors. Knowledge of it is also necessary for athletes, fitness instructors, students and other categories of people. The structure of the hand, as you noticed, is quite complex, and you can study it for quite a long time, relying on various sources.
(articulation radiocarpalis) connects the bones of the forearm and hand. The articular fossa in it is formed by the carpal surface of the radius and the distal surface of the articular disc. The articular head is the bones of the proximal row of the wrist. The joint capsule is strengthened by the radial and ulnar collateral ligaments, the palmar and dorsal radiocarpal ligaments, and the ligaments that connect the individual bones of the wrist on the palmar and dorsal sides. The joint is elliptical in shape.Movements:
Around the frontal axis: flexion/extension of the hand
Around the sagittal axis: adduction/abduction of the hand.
Flexors:
flexor carpi radialis and ulnaris,
Palmaris longus muscle.
Extensors:
Long and short radial and ulnar extensor carpi muscles.
Lead:
Extensor carpi radialis brevis and longus,
flexor carpi radialis
Abductor pollicis longus muscle
Extensor pollicis longus and brevis.
Blood supply of the HP: arterial network formed by the branches of the radial, ulnar, interosseous anterior and posterior arteries.
Intercarpal joints, articulatio nesintercarpeae, connect the bones of the wrist. These joints are strengthened by interosseous and intercarpal ligaments, ligamemainte-rosseaetintercarpea, palmar and dorsal intercarpal and, ligamenta intercarpeapalmariaeidorsalea.
Midcarpal joint , articulatio mediocarpalis, located between the proximal and distal rows of carpal bones
· Midcarpal joint, is located between the first and second rows of carpal bones, minus the pisiform bone. Formed by the distal surface of the first row of carpal bones and the proximal surface of the second row of carpus.
· Articulation of the pisiform bone, represents a separate joint in which the pisiform bone articulates with the triquetral bone.
· Flexor retinaculum, is not directly related to the joints of the hand; it spreads in the form of a bridge from the radial eminence of the hand to the ulnar eminence of the hand through the carpal groove, turning the latter into the carpal canal.
· Carpometacarpal joints, formed by the second row of carpal bones and the bases of the metacarpal bones. With the exception of the carpometacarpal joint of the thumb, all these joints are flat, reinforced both from the rear and from the side of the palm by tightly stretched ligaments, the mobility in them is extremely insignificant.
· Metacarpophalangeal joints, between the convex heads of the metacarpal bones and the fossae at the base of the proximal phalanges, ellipsoid. Movements are performed around two axes: frontal - flexion and extension of the entire finger and sagittal - abduction and adduction of the finger; Roundabout Circulation.
· Interphalangeal joints, located between the head and base of adjacent phalanges, these are trochlear joints that produce flexion and extension around the transverse axis.
Wrist joint and joints of the hand bones
Wrist joint, articulatio radiocarpalis. The joint is formed by the carpal articular surface of the radius, on the medial side by the articular disc, discus articulars, and by the proximal surfaces of the first (proximal) row of carpal bones: scaphoid, lunate, triquetrum (Fig. 88).
The bones of the wrist, located between the bones of the forearm, on the one hand, and the metacarpal bones, on the other, play an important role as a connecting link, providing a variety of movements of the most complex and important part of the upper limb - the hand. They are part of several joints:
radiocarpal, midcarpal, intercarpal and carpometacarpal.
The structure of the wrist joint is complex, and the shape of the articular surfaces is ellipsoidal with two axes of movement - frontal and sagittal.
The articular capsule is thin, especially at the back, and is attached to the edges of the articular surfaces of the articulating bones. On the radial side, the articular capsule is supported by the radial collateral carpal ligament, Ug. collaterale carpi radiate, running from the styloid process of the radius to the scaphoid (Fig. 89). The ulnar collateral ligament located on the ulnar side, Ug. collaterale carpi ulndre, stretched between the styloid process of the ulna on one side, the triquetral and pisiform bones on the other. On the palmar and dorsal surfaces of the wrist joint are the palmar and dorsal radiocarpal ligaments, respectively.
Palmar radiocarpal ligament, Ug. radiocarpale palmare, starts from the anterior edge of the articular surface of the radius, is attached by separate bundles to the bones of the first row of the wrist and to the capitate bone of the second (distal) row. Dorsal radiocarpal ligament, lig. radiocarpale dorsale, goes from the radius exclusively to the first row of carpal bones.
Midcarpal joint, articulatio mediocarpalis. It is located between the bones of the first and second rows of the wrist and is functionally connected to the wrist joint. The articulating surfaces of this joint have a complex configuration, and the joint space is S-shaped. Thus, there are, as it were, two heads in the joint, one of which is formed by the scaphoid bone, and the second by the capitate and hamate bones. The first articulates with the trapezium and trapezoid bones, the second with the triquetrum, lunate and scaphoid bones. The articular capsule of the midcarpal joint is relatively loose and very thin on the dorsal side. The cavity of the midcarpal joint continues between the bones that form the first and second rows of the wrist, i.e., it connects with the cavities of the intercarpal joints.
Intercarpal joints, articulationes infercarpales. These joints are located between the individual bones of the wrist. They are formed by the surfaces of articulating bones facing each other.
The midcarpal and intercarpal joints are strengthened by the palmar and dorsal ligaments. On the palmar surface is the radiate carpal ligament, Ug. carpi radiatum, which are bundles of fibers diverging from the capitate bone to adjacent bones. The palmar intercarpal ligaments, Ugg, are also located here. intercdrpalia palmdria, and on the back - dorsal intercarpal ligaments, ligg. intercarpalia dorsalia. They go from one bone to another, mainly in the transverse direction. The individual bones of the wrist are also connected to each other by intra-articular ligaments. These are interosseous intercarpals with v i zk i. iigg- intercarpalia interossea.
The intercarpal joint also includes the joint between the pisiform and triquetral bones - the joint of the pisiform bone, articulatio ossis pisiformis, reinforced by the pisiform-hook ligament, lig. pisohamdtum, and pisiform-metacarpal ligament, lig. pisometacarpale, which ends at the base of the IV-V metacarpal bones. Both ligaments are a continuation of the flexor carpi ulnaris tendon.
Carpometacarpal joints, artICulatIOnes carpometacdrpales.
These joints are formed by the distal articular surfaces of the second row of carpal bones and the articular surfaces of the base of the metacarpal bones.
The carpometacarpal joint of the thumb, articulatio carpometacarpalis pollicis, differs in shape from the rest and is a typical saddle joint, and the carpometacarpal joints of the II-V fingers are flat joints.
The carpometacarpal joint of the thumb is completely isolated from the other carpometacarpal joints and has significant mobility. The wide articular capsule and saddle-shaped articular surfaces allow movements in this joint around two axes: sagittal, passing through the base of the first metacarpal bone, and frontal, passing through the trapezium bone. The frontal axis is located at a certain angle to the frontal plane, i.e., not strictly transverse. Around it, flexion and extension of the thumb along with the metacarpal bone are possible. Due to the fact that the axis is not completely transverse, the thumb, when bent, moves towards the palm, opposed to the rest of the fingers. Reverse movement of the thumb - returning the finger to its original position. Movement around the sagittal axis - adduction and abduction of the thumb to the index (II) finger. Circular movement is also possible in this joint as a result of a combination of movements around the two named axes.
The carpometacarpal joints of the II-V fingers, articulationes carpometacarpdies II-V, are formed by the articulation of the articular surfaces of the second row of carpal bones with the base of the II-V metacarpal bones. Their common joint space is a transverse broken line. The articular capsule is relatively thin, common to all four joints and tightly stretched, and the articular cavity is connected to the cavities of the midcarpal and intercarpal joints. On the dorsal and palmar sides, the capsule is strengthened by strong ligaments - these are the dorsal carpometacarpal ligaments, ligg. carpometacarpalia dorsalia, and palmar carpometacarpal ligaments, ligg. carpometacarpalia palmdria.
Intermetacarpal joints, articulationes intemetawrpales. The joints are formed by the adjacent surfaces of the bases of the II-V metacarpal bones. The capsule of these joints is common with the capsule of the carpometacarpal joints and is strengthened by the dorsal and palmar metacarpal ligaments, ligg. metacarpdlia dorsalia et palmdria, which run transversely and connect adjacent metacarpal bones. There are also interosseous metacarpal ligaments, ligg. metacarpalia interossea, lying inside the joints and connecting the surfaces of the metacarpal bones facing each other.
The movements of the hand relative to the forearm involve the wrist, midcarpal, carpometacarpal joints, as well as the intercarpal and intercarpal joints. All these joints, united by a single function, are often called the carpal joint by clinicians. The total range of motion of the hand is the sum of the movements in all these joints. The wrist joint is an ellipsoidal joint, in which movements around the frontal (flexion and extension of the hand) and sagittal (abduction and adduction of the hand) axes are possible. The midcarpal joint, although it consists of two joints seemingly connected into one spherical joint, is shaped like a trochlear joint due to the irregular shape of the articular surfaces. In this joint, movement is possible only around the frontal axis - flexion and extension. The range of movements simultaneously in the wrist and intercarpal joints during flexion is 75-80°, during extension - about 45°, during abduction - 15-20°, adduction 3040°. Circular motion in these joints is the result of the addition of successive movements around the sagittal and frontal axes. The ends of the fingers of the hand describe a circle.
The carpometacarpal joints are flat, reinforced by strong and tightly stretched ligaments, and have extremely little mobility. In the intercarpal and intermetacarpal joints, only a slight displacement of the bones relative to each other occurs during flexion and extension movements of the hand. Firmly connected to each other and to the II-V metacarpal bones, the bones of the second row of the wrist mechanically form a single whole - the solid base of the hand. For all movements in the joints of the wrist, their center can be considered the head of the capitate bone, and the proximal row of carpal bones plays the role of a bony meniscus.
Metacarpophalangeal joints, articulationes metacarpophalangedles. The joints are formed by the articular surfaces of the heads of the metacarpal bones and the bases of the proximal phalanges. The articular surfaces of the heads are rounded, and the articular cavities of the proximal phalanges are ellipsoidal. The joint capsules are free and strengthened on the sides by collateral ligaments, ligg. collaterdlia. On the palmar side, the capsule is thickened due to bundles of fibers of the palmar ligaments, ligg. palmdria. In addition, the metacarpophalangeal joints of the II-V fingers are strengthened by transversely running fibers located between the heads of the metacarpal bones and forming deep transverse metacarpal ligaments, ligg-metacarpalia transversa profunda.
In the metacarpophalangeal joints, movements around two axes are possible. Around the frontal axis, flexion and extension are carried out with a range of motion of about 90°. Abduction and adduction of the fingers occur around the sagittal axis (the total range of motion of one finger is 45-50°). Circular movements are also possible in these joints.
Interphalangeal joints of the hand, articulationes interphalangeales manus. The head and base of the adjacent phalanx are involved in the formation of the joint. All joints are built identically and are typical block-shaped in shape of the articular surfaces. The capsule of each joint is free, on the sides it is strengthened by collateral ligaments, ligg. collateralia. On the palmar side, the capsule is thickened due to the palmar ligaments, ligg. palmdria. In these joints, movements are possible only around the frontal axis - flexion and extension (total range of motion is about 90°).
X-ray anatomy of the hand joints
An x-ray examination of the hand clearly shows the articulating bones and x-ray joint spaces of all joints (Fig. 90). The X-ray joint space of the wrist joint is widened at the medial edge due to<прозрачности>for X-raying of the articular disc at the head of the ulna. Only the pisiform bone overlaps the triquetrum; the remaining bones of the wrist are visible separately, as a result of which the joint spaces between them are clearly contoured. X-ray joint spaces of the metacarpophalangeal and interphalangeal joints are directed distally with their convex side.
flexor carpi radialis,T.flexor carpi radialis. Function: flexes the wrist. Innervation: n. medianus. Blood supply: a. brachialis, a. ulnaris, a. radialis.
Abductor pollicis brevis muscle, m. fabductor pollicis brevis. Function: abducts the thumb. Innervation: n. medianus. Blood supply: r. palmaris superficialis, a. radialis
Muscle opposite the thumb, m. opronens pollicis. Function: contrasts the thumb with the little finger and all other fingers of the hand. Innervation: n. medianus. Blood supply: r. palmaris superficialis, a. radialis, arcus palmaris profundus.
Shortflexorbigfingerbrushes, m. flexor pollicis brevis. Function: flexes the proximal phalanx of the thumb and the finger as a whole. Innervation: n. ulnaris, n. medianus. Blood supply: r. palmaris superficialis, a. radialis.
Adductor pollicis muscle, m. abductor pollicis. Function: brings the thumb to the index finger, participates in flexion of the thumb. Innervation: n.ulnaris. Blood supply: arcus palmeris superficialis et arcus palmaris profundus.
Longflexorbigfingerbrushes, m. flexor pollicis longus. Function: flexes the distal phalanx of the thumb, flexes the hand. Innervation: n. medianus. Blood supply: a. interossea anterior
The most complete answers to questions on the topic: “wrist joint description according to the algorithm.”
Radiocarpal joint(lat. articulátio radiocárpea) - a movable connection of the bones of the human forearm and hand. Formed by the expanded and concave carpal articular surface of the radius and the distal (located further from the body) surface of the triangular cartilaginous disc, representing a concave articular surface articulating with the convex proximal (located closer to the body) articular surface of the bones of the first row of the wrist: scaphoid, lunate and triquetrum.
According to the number of bones involved, the joint is complex, and according to the shape of the articular surfaces it is classified as ellipsoid (lat. articulacio ellipsoidea) with two axes of rotation (sagittal and frontal). The following movements are possible in the joint:
- sagittal axis - abduction and adduction of the hand;
- frontal axis - flexion and extension;
- the ellipsoidal shape of the joint allows for circular rotation of the hand (lat. circumductio).
Anatomy
In the process of evolution, as the ability to pronate and supinate is acquired, the block-shaped joint of mammals is supplemented by a distal radioulnar joint (lat. articulatio radioulnáris distális), which, together with the proximal radioulnar joint (lat. articulatio radioulnáris proximális) forms a single combined articulation with a vertical axis rotation. In humans, due to the greatest volume of rotation of the forearm, the articular disc (lat. discus articuláris) of the distal epiphysis of the ulna reaches its highest development and takes the form of a triangular fibrocartilaginous plate, forming the articular cavity of the proximal wrist joint. Thus, the ulna participates in the wrist joint only through the aforementioned cartilaginous disc, without being directly related to this articulation. Therefore, the joint is called not the antebrachial, but the radiocarpal.
Articular surfaces: the articular cavity is formed by the radius and a triangular cartilaginous disc, attached between the radius and the styloid process of the ulna, and the articular head is the proximal surface of the first row of carpal bones (scaphoid, lunate and triquetrum), connected by interosseous ligaments (lat. ligaméntum intercárpea) .
The joint capsule is thin, attached to the edges of the articular surfaces of the bones that form the joint.
The joint is held in place by ligaments:
- The lateral radial ligament of the wrist (lat. ligaméntum collaterále cárpi radiále) - between the styloid process of the radius and the scaphoid bone - limits the adduction of the hand;
- The lateral ulnar ligament of the wrist (lat. ligaméntum collaterále cárpi ulnáre) - between the styloid process of the ulna and the triquetral bone (some of the fibers reach the pisiform) - limits the abduction of the hand;
- The dorsal radiocarpal ligament (lat. ligaméntum radiocarpéum dorsále) - between the dorsal surface of the distal epiphysis of the radius and the dorsal surfaces of the carpal bones (scaphoid, lunate and triquetrum) - limits the flexion of the hand;
- The palmar radiocarpal ligament (lat. ligaméntum radiocarpéum palmáre) - between the base of the styloid process of the radius and the bones of the first (scaphoid, lunate and triquetrum) and second (capitate bone) rows of the wrist - limits the extension of the hand;
- Intercarpal interosseous ligaments (lat. ligaménta intercárpea interóssea) - connecting the bones of the first row of the wrist.
Blood supply
Réte articulare- arterial network formed by branches of a. radialis, a. ulnaris, aa. interósseae. On the palmar surface of the ligamentous apparatus of the wrist there are anastomoses of the palmar carpal branches of the radial and ulnar arteries, as well as branches of the deep palmar arch and the anterior interosseous artery.
Venous drainage
It is carried out from the deep palmar venous arch of the wrist into the deep veins of the upper limb, two accompanying arteries of the same name: ulnar veins (lat. vv. ulnáres), radial veins (lat. vv. radiáles), interosseous veins (lat. vv. interósseae).
Lymphatic drainage
It is carried out through deep lymphatic vessels into the palmar lymphatic plexus, then into the lymph nodes of the ulnar fossa of the lats. nódi limphátici cubitáles.
Innervation
Brachial plexus: radial nerve (lat. n. radiális), ulnar nerve (lat. n. ulnáris), median nerve (lat. n. mediális).
Channels
In the area of the wrist joint there are three canals formed by the flexor retinaculum (lat. retináculum flexórum) in the groove (lat. súlcus cárpi) between the ulnar (lat. eminéncia cárpi ulnáris) and radial (lat. eminéncia cárpi radiális) protrusions:
- cubital canal (lat. canális cárpi ulnáris) - contains the ulnar nerve and vessels from the groove (lat. súlcus ulnáris) of the forearm (ulnar artery and veins);
- radial canal (lat. canális cárpi radiális) - contains the tendon of the radial flexor carpi and the radial artery;
- carpal tunnel (lat. canális carpális) - contains two separate synovial sheaths (for the tendons of the superficial and deep flexor digitorum and the second for the tendon of the flexor pollicis longus), the median nerve and the artery accompanying the median nerve (ulnar artery system).
Pathology
Inflammatory processes
Arthritis
Additional information:
Arthritis of the wrist joint- acute or chronic inflammatory process, characterized by pain and impaired mobility (feeling of stiffness). The joint area becomes swollen, red and hot to the touch. Depending on the reason, there are:
- specific arthritis, developing as a complication of tuberculosis, syphilis, gonorrhea;
- nonspecific arthritis, caused by the penetration of pyogenic microorganisms into the joint cavity with the flow of blood or lymph from the main purulent focus or as a result of the penetration of infectious agents from the outside during a penetrating wound of the joint;
- infectious-allergic arthritis- the result of immune autoaggression against the background of infectious diseases (brucellosis, measles and others);
- against the background of systemic connective tissue diseases: rheumatoid arthritis (characteristically symmetrical joint damage) and joint damage in systemic lupus erythematosus;
- as a result of salt deposition against the background of metabolic disorders (for example, gout).
Treatment depends on the stage and nature of the inflammatory process.
- In case of acute purulent inflammation, surgical drainage of the joint cavity is performed for free outflow of pus and antibacterial therapy.
- In case of chronic or specific arthritis, the joint is immobilized in a physiologically advantageous position, and nonspecific anti-inflammatory and specific antibacterial therapy is prescribed (depending on the etiology of the pathogen).
- Against the backdrop of the subsidence of the inflammatory process, physical therapy, massage, and physiotherapeutic methods of treatment are included.
- In the remission stage of chronic arthritis, it is recommended to take hodroprotectors to restore joint tissue, continue physical therapy, control the load on the joint, and follow dietary recommendations (Gout).
Untimely and improper treatment of arthritis of the wrist joint leads to the development of deforming osteoarthritis with a decrease in its motor function up to ankylosis.
Osteoarthritis
Osteoarthrosis of the wrist joint- degenerative-dystrophic disease of the joint, which develops as a result of damage to the cartilage tissue of the articular surfaces. Pathologies of large joints (hip, knee and ankle) are much less common, but they represent a serious problem associated with limitations in work activity and self-care. The cause of osteoarthritis of the wrist joint can be age-related degeneration of cartilage, systematic overload and microtraumatization of the joint (painters, musicians, typists, PC operators and artists), trauma or inflammatory processes.
Clinical picture: limitation of mobility and pain, aggravated by palpation or passive movements in the joint against the background of crunching and clicking, not observed in healthy people. As the process progresses, the pain syndrome intensifies, and the range of motion in the joint decreases - stiffness develops.
Treatment aimed at relieving pain - long-term immobilization of the joint in a physiologically advantageous position using special bandages or orthoses, prescribing non-steroidal anti-inflammatory drugs. Drug therapy is complemented by physiotherapeutic methods and spa treatment in orthopedic sanatoriums. In cases where the pain syndrome cannot be relieved, intra-articular injections of glucocorticoids or surgical treatment aimed at creating artificial ankylosis are used (stiffness in the joint relieves the patient of pain). Treatment tactics in each specific case can only be chosen by a doctor based on the clinical picture and X-ray data.
More articles: Polyarthritis of the shoulder joint
Injuries
Injuries (bruise, dislocation, fracture, sprain) most often occur as a result of direct exposure to force during bruises and falls with emphasis on the palm. Injuries to the wrist bones should be taken extremely seriously, as incorrect and untimely treatment can lead to loss of function.
Fracture
Among the bones of the wrist, the scaphoid bone and, less commonly, the lunate bone are subject to fracture:
- Clinical picture- a painful swelling appears, most pronounced on the dorsal surface of the wrist joint, movements are limited, pain intensifies with load along the axis of the outstretched fingers.
- Diagnostics- is based on anamnesis and objective research. X-ray examination allows you to verify the diagnosis.
- Treatment- immobilization in the average physiological position of the hand and forearm using a plaster splint for up to 6 weeks due to the low intensity of blood supply to the bones of the wrist.
Injuries
Additional information:
Wounds of the wrist joint (puncture, laceration, bruised-laceration, cut, chopped up to traumatic amputation, crushing, bitten, but more often gunshot) are rare.
First aid- stopping bleeding (tourniquet or digital pressure of the vessel), applying an aseptic dressing, immobilization (fixation) of the hand and forearm using improvised means. To prevent tetanus in an outpatient or hospital setting, antitetanus serum is administered according to Bezredka. In a hospital setting, primary surgical treatment of the wound is performed, the final stop of bleeding, removal of necrotic tissue, bone fragments and other artifacts, after which fixation with a plaster cast is performed from the metacarpophalangeal joint to the middle third of the shoulder in a functionally advantageous position of the elbow and wrist joint. Primary surgical treatment of open injuries of the wrist joint is mandatory to prevent the occurrence of purulent complications of damage to the wrist joint, as well as (in the long term) the development of osteomyelitis.
Bone age
The skeleton of the hand and wrist joint is the most convenient object for x-ray studies of the development of the human skeletal system. An X-ray of the hand and wrist joint in a direct projection shows the ossification nuclei of the carpal bones, the distal epiphyses of the radius and ulna, and the presence of synostosis of the epiphyses and diaphyses. The timing of the appearance of ossification nuclei and synostosis depends on gender and age. The technique is used to determine biological age and its correspondence to passport age.
In a full-term newborn, an X-ray examination of the hand and wrist joint in a direct projection reveals ossification of the diaphyses of the tubular bones (developed from the main points of ossification starting from the second month of the child’s intrauterine development); the epiphyses of the tubular bones and the bones of the wrist are at the cartilaginous stage of development, therefore they are not visualized in the image . Sometimes an x-ray of a newborn reveals ossification points of the capitate and hamate bones, which further confirms that the newborn is full-term. Subsequently, there is a sequential appearance of ossification nuclei in the bones of the wrist and the epiphyses of the tubular bones. The onset of synostosis of the epiphyses and diaphysis of tubular bones in men occurs at the age of 19-23 years, in women at 17-21 years. Modern studies indicate earlier periods of synostosis (closure of cartilaginous growth zones). The skeleton of the wrist joint and hand, consisting of a large number of bones, undergoes significant age-related changes. Knowledge of the timing and sequence of appearance of ossification nuclei allows professionals to determine the presence of endocrine pathology and diseases of other body systems.
Notes
- Wrist joint- article from the Great Soviet Encyclopedia.
- R. D. Sinelnikov. Atlas of human anatomy. - 3rd ed., revised. and additional - M.: Medicine, 1967. - T. I. - P. 207. - 460 p. - 105,000 copies.
- Human anatomy / Prives M. G., Lysenkov N. K. - 9th ed., revised. and additional - M.: Medicine, 1985. - P. 131-132. - 672 s. - (Educational literature for students of medical institutes). - 110,000 copies.
- R. D. Sinelnikov. Atlas of human anatomy. - 4th ed., revised. and additional - M.: Medicine, 1973. - T. II. - P. 319. - 468 p. - 165,000 copies.
- R. D. Sinelnikov. Atlas of human anatomy. - 4th ed., revised. and additional - M.: Medicine, 1973. - T. II. - P. 394. - 468 p. - 165,000 copies.
- R. D. Sinelnikov. Atlas of human anatomy. - 4th ed., revised. and additional - M.: Medicine, 1973. - T. II. - P. 454. - 468 p. - 165,000 copies.
- R. D. Sinelnikov. Atlas of human anatomy. - 3rd ed., revised. and additional - M.: Medicine, 1967. - T. III. - pp. 192-210. - 394 s. - 50,000 copies.
- Human anatomy / Prives M. G., Lysenkov N. K. - 9th ed., revised. and additional - M.: Medicine, 1985. - P. 213. - 672 p. - (Educational literature for students of medical institutes). - 110,000 copies.
- Human anatomy in two volumes / Ed. acad. RAMS prof. M. R. Sapina. - 5th ed., revised. and additional - M.: Medicine, 2001. - T. I. - P. 404-405. - 640 s. - (For medical students, graduate students, doctors). - ISBN 5-225-04585-5.
- Arthritis of the wrist joint.
- Pokrovsky V.I. Small medical encyclopedia. - Soviet Encyclopedia, 1996. - T. 4. - 577 p. - ISBN 5-225-02819-5.
- Arthrosis of the wrist joint.
- Surgical diseases in children / Ed. Yu. F. Isakova. - 1st ed. - M.: Medicine, 1993. - P. 387-388. - 576 p. - (Educational literature for students of medical institutes). - 15,000 copies. - ISBN 5-225-00875-5.
- Medical encyclopedia: Wrist joint
- Human anatomy / Prives M. G., Lysenkov N. K. - 9th ed., revised. and additional - M.: Medicine, 1985. - P. 130-131. - 672 s. - (Educational literature for students of medical institutes). - 110,000 copies.
The wrist joint includes:
- radius;
- wrist bones;
- joint cartilage;
- capsule.
Anatomy of the wrist joint
Articular cartilage is similar to a triangle. An important part of it is the ligaments. They connect the bones and give the joint stability. The wrist joint includes the lateral radial ligament, lateral ulnar ligament, dorsal radiocarpal ligament, palmar ligament, and intercarpal ligament.
The capsule is wide and quite thin. It is attached below to the upper bones of the wrist, and above to the articular disc and radius. The joint moves due to the work of muscles. On the back of the hand there are extensors of the hands and fingers, on the side of the palm there are flexors.
The wrist joint is complex in the number of bones connected to each other. Its shape is similar to an ellipse with 2 axes of rotation. The following movements are available to the joint:
- abduction and adduction of the hand;
- flexion and extension.
Thanks to this folding of the joint, rotation is also possible. High mobility is possible due to the large number of bones in the joint structure. But this property also has a negative side, because it increases the risk of injury.
Joint structure
Due to the development and ability to pronate (movement of the arm inward) and supination (movement of the arm outward), people have another joint; together with the proximal joint, it forms the overall structure. This makes it possible to implement movements with a maximum amplitude of rotation of the forearm. The articular disc is a fibrocartilaginous plate with a triangular shape that originates from the distal epiphysis of the elbow bone and complements the glenoid cavity of the proximal part of the wrist joint. This plate gives the articular plane congruency, allowing the surfaces to correspond to each other.
More articles: Recovery exercises after hip replacement
The wrist joint has a number of joints that make it possible to perform various movements.
The wrist joint contains two articular planes:
proximal – radius and cartilaginous disc;
distal - proximal plane of the small bones of the first row of the wrist (scaphoid, lunate, triangular, united by fibers).
The joint is covered with a thin capsule and is attached to the bone tissue along the edges of the bones that form the joint.
Strengthening the wrist joint is performed by the following ligaments:
Radial collateral ligament - placed between the styloid process of the radius and the scaphoid bone. Limits excessive adduction of the hand.
Ulnar collateral ligament - placed between the styloid process of the ulna and the triangular bone. Limits excessive hand abduction.
Palmar ulnocarpal ligament - originates from the articular disc and styloid process of the ulna, descends downward and inward, attaches to the triangular, lunate and capitate bones. This ligament strengthens both the wrist joint and the midcarpal joint.
Dorsal radiocarpal ligament - starts from the back edge of the distal epiphysis of the radius, passes to the wrist and is attached to the back of the lunate, scaphoid and triangular bones. Protects against excessive flexion of the hand.
Palmar radiocarpal ligament - located among the styloid process of the radius, goes down and to the center, attaches to the bones of the first and second rows of the wrist.
Interosseous ligament – unite single bones of the 1st row of the wrist.
The structure of the wrist joint gave it the following characteristic features:
the articulation is complex in structure, it is formed by more than two articular planes;
complex articulation - the joint capsule contains additional cartilaginous components to ensure congruence;
ellipse shape - made up of bone planes, which are segments of an ellipse (one plane is convex and the other is concave).
The ellipsoidal type of articulation makes it possible to move around two axes: around the frontal (extension and flexion) and sagittal (abduction and adduction).
In the wrist joint there are channels with blood vessels and nerves.
There are three channels:
Ulnar canal – includes artery, veins and nerve.
Radial canal – includes the flexor carpi radialis tendon and artery.
Carpal tunnel - includes the artery and median nerve and the tendons of the flexor muscles of the fingers.
What does the wrist joint consist of?
The wrist joint is the connection between the forearm and the hand. The wrist joint is formed by the radius and the carpal bones - the scaphoid, lunate and triquetrum. It allows movements: flexion and extension, adduction and abduction of the hand. The capsule of the wrist joint with its upper edge is attached to the radius and triangular cartilage, and its lower edge is attached to the first row of carpal bones. On the palmar surface of the wrist joint there are two synovial sheaths. through which the finger flexor tendons pass, arranged in four layers.
The extensor tendons at the level of the wrist joint are located in the synovial sheaths and are located on the dorsum of the wrist joint in two layers. The blood supply to the palmar side of the wrist joint comes from the radial and ulnar arteries, each of which is accompanied by two veins. The dorsum of the wrist joint receives blood from the dorsal branch of the radial artery. The joint is innervated by the branches of the ulnar and median nerves. Lymphatic drainage is carried out by deep lymphatic vessels into the axillary lymph nodes.
Right hand cut:
1 - interosseous membrane;
2 - radius;
3 - wrist joint;
4 - scaphoid bone;
5 and 12 - lateral radial and ulnar ligaments of the wrist;
6 and 7 - small and large trapezoid bones;
8 - metacarpal bones;
9 - capitate bone;
10 - hamate bone;
11 - triangular bone;
13 - articular disc;
14 - ulna.
Damage. Bruises of the wrist joint are relatively rare. A sprain occurs with sudden excessive flexion, extension, abduction and adduction of the hand and is accompanied by tearing of the ligaments. In this case, swelling and pain during movement are detected in a limited area of the wrist joint. The diagnosis of sprain is made only after excluding a fracture of the radius and scaphoid bones. Treatment: cold, pressure bandage or dorsal plaster splint on the hand and forearm for 3-6 days.
Dislocations in the wrist joint are extremely rare; dislocations of the lunate or scaphoid are more common. First aid for sprains comes down to applying an immobilizing bandage such as a scarf. Treatment - reduction of the dislocation - is performed by a doctor under anesthesia; After reduction, a plaster splint is applied for 3 weeks. Then thermal procedures and therapeutic exercises are prescribed.
Of the intra-articular fractures of the bones of the wrist joint, fractures of the scaphoid and lunate bones are most common. A fracture of the scaphoid bone occurs when falling on an outstretched arm, and can be combined with a fracture of the radius in a typical location (see Forearm). Symptoms: swelling, pain and difficulty moving the wrist joint. The diagnosis is clarified radiographically. Treatment: application of a plaster splint for 8-10 weeks. Subsequently, therapeutic exercises are performed to develop the function of the joint. thermal procedures.
Wounds to the wrist joint (most often gunshot) are rarely observed in peacetime. First aid consists of applying an aseptic bandage, immobilizing the limb, and administering antitetanus serum according to Bezredka. In a surgical hospital - primary wound treatment. stopping bleeding, removing bone fragments, etc.; then apply a plaster cast from the metacarpophalangeal joint to the middle third of the shoulder in a functionally advantageous position of the elbow and wrist joint. Primary treatment of open injuries of the wrist joint prevents the further development of purulent complications in the wrist joint, as well as (in later stages) osteomyelitis.
Diseases. Arthritis of the wrist joint occurs primarily as a complication of purulent tenobursitis as a result of penetrating wounds or tuberculosis infection (see Arthritis, Tuberculosis of bones and joints).
The wrist joint (articulatio radiocarpea) connects the forearm to the hand. This articulation involves the radius and the proximal row of carpal bones - the scaphoid (os scaphoideum), lunate (os lunatum) and triquetrum (os triquetrum). Between the first and second rows of carpal bones there is an intercarpal joint, which, together with the radiocarpal joint, forms a functionally interconnected joint of the hand. The glenoid cavity is formed by the carpal articular surface of the radius (facies articularis carpea radii), which connects to the scaphoid and lunate bones, as well as triangular connective tissue cartilage (discus articularis), which fills the space between the ulna, which is shorter than the radius, and is the articular surface for a triangular bone. The distal ends of the radius and ulna are connected by an articulation (art. radioulnaris distalis).
The wrist joint capsule is very thin. Its upper edge is attached to the edge of the articular surface of the radius and triangular cartilage, the lower - to the edge of the articular surfaces of the first row of carpal bones. The joint capsule is strengthened laterally by the radial collateral carpal ligament (lig. collaterale carpi radiale) and the ulnar lateral carpal ligament (lig. collaterale carpi ulnare). In addition, the palmar radiocarpal ligament (lig. radiocarpeum palmare) is stretched from the radius to the bones of the wrist from the palmar surface. The same ligament (lig. radiocarpeum dorsale) is also present on the dorsal side (Fig. 1 and 2). The capsule of the wrist joint is fed from the vessels that form the rete carpi palmare (see Hand).
On the palmar surface of the wrist joint there are two synovial sheaths, in which the finger flexor tendons pass under the retinaculum flexorum - a dense ligament that is a continuation of the palmar aponeurosis. The main muscles that flex the hand are the radial and ulnar flexors of the wrist (hand) and the long palmar muscle (mm. flexor carpi radialis, palmaris longus et flexor carpi ulnaris). Extension of the hand is performed by the long and short radial extensors of the wrist (hand) and the extensor ulnaris (mm. extensores carpi radiales longus et brevis et m. extensor carpi ulnaris). The extensor tendons at the level of the wrist joint are located in the sheaths and pass under the retinaculum extensorum. On the palmar surface of the L.-z.s. tendons and muscles are arranged in four layers, on the back - in two layers. In addition to the indicated muscles of the flexors and extensors of the hand, other muscles have an indirect effect on the function of the joint.
More articles: Rehabilitation of the spine and joints
The joint receives blood supply from the palmar side from the radial and ulnar arteries. The radial artery is accompanied by two veins and is located superficially. The ulnar artery runs in the ulnar groove of the forearm, accompanied by two veins. The ulnar nerve is located medial to the artery. The median nerve passes along the palmar surface of the wrist joint along with the flexor tendons. Unlike tendons, which have a lamellar structure when cut, the median nerve has a cable structure (consists of individual longitudinal fibers). This is important to remember when suturing the ends of damaged tendons and nerves. The back surface of the L.-z.s. receives blood supply from the dorsal branch of the wrist of the radial artery (ramus carpeus dorsalis) and the dorsal arterial network of the L.-z.s. (rete carpi dorsale).
L.-z.s. is an ellipsoidal biaxial joint that allows movements in the sagittal and frontal planes of the hand.
Source: www.medical-enc.ru
Function of the muscles of the wrist joint
Classically, the main muscles of the wrist joint are divided into four groups, and in Fig. 138 (cross section) schematically shows how they are related to the two axes of the wrist joint: the flexion/extension axis AA′ and adduction/abduction axis BB′ .
(The diagram shows a frontal section through the distal part of the wrist joint: IN'- front view, IN- back view, A'- outside view, A- inside view. The tendons of the muscles that carry out movements in the wrist joint are shown in gray; the tendons of the finger muscles are shown in white.)
Group I - flexor carpi ulnaris1:
- performs flexion in the wrist joint (being in front of the axis AA′) and in the carpometacarpal joint of the fifth finger due to tendon stretching;
- leads the hand (being in front of the axis BB′), but weaker than the extensor carpi ulnaris.
An example of adduction flexion is the position of the left hand when playing the violin.
Group II - extensor carpi ulnaris:
- extends the wrist joint (being posterior to the axis AA′);
- adduces the hand (being medial to the axis BB′).
Group III - flexor carpi radialis2 and palmaris longus:
- bend the wrist joint (being in front of the axis AA′);
- BB′).
Group IV - extensor carpi radialis longus4 and extensor carpi radialis brevis:
- extend the wrist joint (being behind the axis AA′);
- retract the hand (being outside the axis BB′).
According to this theory, none of the muscles of the wrist joint has only one action. Thus, in order to perform any one movement, it is necessary to activate two muscle groups in order to suppress unwanted associated movements (this is another example of muscle antagonism-synergism).
- Flexion(FLEX) requires activation of muscles I (flexor carpi ulnaris) and III (flexor carpi radialis and palmaris longus) muscles.
- Extension(ECT) requires the participation of muscles II (extensor carpi ulnaris) and IV (extensor carpi longus and brevis) groups.
- Bringing(ADD) is carried out by muscles I (flexor carpi ulnaris) and II (extensor carpi ulnaris) groups.
- Lead(ABD) is carried out by muscles III (flexor carpi radialis and palmaris longus) and IV (extensor carpi radialis longus and brevis) groups.
However, in practice, the function of each muscle individually is more complex. Usually movements occur in pairs: flexion - abduction; extension - adduction.
Experiments by Duchamp de Boulogne (1867) using electrical stimulation showed the following:
- only the long extensor carpi radialis performs extension and abduction, the short extensor carpi radialis is exclusively an extensor, which indicates its physiological importance;
- Like palmaris longus, the flexor carpi radialis serves exclusively as a flexor, flexing the second metacarpal joint with pronation of the hand. Its electrical stimulation does not produce a lead. During wrist abduction, the flexor radialis contracts only to counterbalance the extensor component of the extensor radialis longus, which is the primary abductor muscle.
Muscles that carry out finger movements. can affect the wrist joint only under certain conditions.
- Finger flexors can flex the wrist joint only if the flexion of the fingers stops before the full excursion of their tendons is completed when these muscles contract. So, if we hold a large object (a bottle) in our hand, the finger flexors help to achieve flexion in the wrist joint. In the same way, the finger extensors take part in the extension of the wrist joint if the fingers are clenched into a fist.
- Abductor pollicis longus muscle and its short extensor abductor carry out abduction in the wrist joint unless they are counteracted by the extensor carpi ulnaris 6. If the latter contracts simultaneously, then under the action of the long abductor only the first finger is abducted. Therefore, the synergistic action of the extensor carpi ulnaris is important for abduction of the thumb, and this muscle can be called the “stabilizer” of the wrist joint.
- Extensor pollicis longus. ensuring its extension and retroposition, can also cause abduction and extension in the wrist joint when the flexor carpi ulnaris is inactive.
- Extensor carpi radialis longus helps to keep the hand in a neutral position, and with its paralysis, its persistent ulnar deviation occurs.
The synergistic and stabilizing effect of the muscles of the wrist joint can be characterized as follows (Fig. 140).
- Extensor muscles of the wrist joint act in synergy with the finger flexors A. For example, when extending the II-V wrist joint, the fingers automatically bend, and in order to straighten them from this position, voluntary effort is required. When the wrist joint is extended, the finger flexors are at their best because their tendons are shorter than when the wrist joint is in neutral or flexed position. Dynamometry shows that the efficiency of the finger flexors in wrist flexion is only 1/4 of their strength in extension.
- Wrist flexors act in synergy with the extensors of the II-V fingers b. When flexing the wrist joint, automatic extension of the proximal phalanges occurs. In order to bend them, voluntary effort is required, and this flexion will be very weak. The tension developed by the finger flexors limits flexion in the wrist joint. When extending the fingers, the amplitude of flexion in the wrist joint increases by 10°.
This delicate muscle balance is easy to upset. Thus, the deformity resulting from an unreduced Coles fracture alters the orientation of the distal radius and articular disc and, by stretching the wrist extensors, reduces the effectiveness of the finger flexors.
Functional position of the wrist joint corresponds to a position that ensures maximum efficiency of the finger muscles, especially the flexors. This position is achieved by slight extension up to 40-45° and slight ulnar deviation (adduction) up to 15°. It is in this position that the hand is most suitable for performing grasping functions.
More articles: A set of exercises after knee replacement
"Upper limb. Physiology of joints"
A.I. Kapandji








- Dihydrotestosterone in men - function, norm and pathology
- Getting insulin: all the main ways
- How steroids affect the prostate gland How to protect the prostate during the course
- Not a virus, not a protein, but its name is prion. Prions for short
- Proper nutrition for stomach ulcers
- Therapeutic back massage for scoliosis Differentiated back massage 10 15
- How to remove phlegm from the bronchi at home
- Cancer neck plant. Snake mountaineer. Cancer neck root
- What are the benefits of kombucha?
- What is dropsy: types and treatment
- Flax seeds for kidney treatment
- How does the influenza virus work?
- Excess protein: how harmful is it?
- Testosterone standards during doping control
- How to correctly use atropine for complex treatment Atropine farm action
- What is hypogonadism in men and how to treat this disease
- The wrist joint is the perfect motor apparatus of the upper limb
- Phosphatidylcholine - fat burning injections
- When is dihydrotestosterone elevated in women and men?
- Diet for thyrotoxicosis of the thyroid gland What foods are not allowed for thyrotoxicosis